





Partnerships and Value
Collaborating for Value: The Path to Successful Academic-Community Relationships
May 30, 2018
11:41 am
Academic medical centers (AMCs) and community health systems are discovering that forming partnership arrangements short of mergers can be an effective strategy for gaining a competitive advantage in their marketplaces.
In the face of numerous market challenges, most healthcare organizations are seeking to enhance their business model by expanding their patient base, securing greater access to advanced technology, and achieving improved economies of scale. AMCs are finding it increasingly challenging to sustain funding for their tripartite mission of patient care, education, and research. Meanwhile, community health systems are seeking to build greater scale, enhance clinical excellence, or simply maintain their identities and find a safe harbor with compatible healthcare partners.
Pushed together by market pressures, these two provider groups are coming together in a variety of business and clinical relationships involving mergers and acquisitions (M&A) and various types of partnerships, such as affiliations, joint ventures, and nonequity alliances. Here, we analyze the various types of academic-community relationships (ACRs) to understand what has worked and what has not, and to identify the key factors associated with success in these new partnerships.
Motivating Factors for Academic-Community Health System Relationships
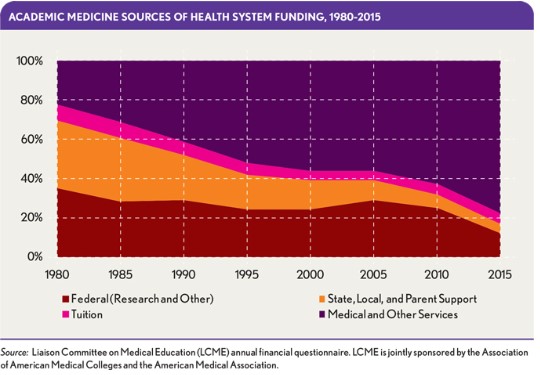
AMCs face unique pressures in needing to maintain sufficient margins not only to be leaders in patient care, but also to teach students, residents, and fellows and encourage clinical research. The funding of academic medicine, in fact, is increasingly reliant on the scale of the health system’s clinical revenue. A recent analysis of AMC revenue sources over time, conducted by the Liaison Committee on Medical Education (LCME), demonstrates that compared with the 1980s, when medical and other clinical services represented only about 20 percent of AMC revenues, that proportion has nearly become inverted, with AMCs now heavily dependent on their clinical health system funding for nearly 80 percent of their revenues, as shown in the exhibit below.
Facing similar market financial pressures, community health systems with strong clinical missions are finding their business model can be best met by affiliation with an academic brand. Of note, 18 of 20 of the U.S. News & World Report’s 2017-18 Best Hospitals Honor Roll have academic sponsorship and university affiliations, and all 20 have substantial teaching and clinical research programs. From a community provider perspective, forging an alliance with a large AMC can yield significant advantages in terms of gaining academic brand awareness and access to exceptional physicians, technology, and new protocols for the treatment of complex and rare diseases.
As AMCs seek to expand their access to clinical activity in the community and community health systems become increasingly avid seekers of academic credentials, the opportunity for establishing creative mutually beneficial collaborations between academic and community provider organizations is favorable. Although simple in concept, crafting the right ACR solution is not easy. Experience has shown that the following challenges and obstacles may be encountered:
- It is easy to underestimate cultural differences between AMCs and community providers.
- Community physicians may view AMC faculty as unwanted competitors.
- There may be a lack of mission alignment if the focus on clinical care ranks third in the AMC’s tripartite mission, given that the community provider’s mission focuses inherently on clinical care.
- AMCs have high cost structures, which may make for problematic partnerships for low-cost population health contracting.
- AMC decision making is complex, and agreements reached at the C-suite level can frequently be contradicted by independent- minded department chairs who are accustomed to control.
To be able to build a relationship that will last and realize the expectations of both participants, both sides should understand the risks and benefits involved in an ACR.
A Range of Relationships
To understand what types of arrangements between AMCs and community health systems work well and what factors are associated with good outcomes, it is helpful to examine the range of relationships currently being pursued in the following four major categories of such arrangements, including three types of ACRs.
Mergers and acquisitions. AMCs have increasingly engaged in M&A activity over the past decade in efforts to find optimum scale, expand the patient base for their operations, and increase clinical margins. After a few years, many of these deals have shown positive outcomes in terms of improved access to capital, cost efficiencies, and increased market share. But higher operating margins have not immediately followed for all the acquisitions, according to a recent research report from HFMA and the Deloitte Center for Health Solutions. In many instances, acquired hospitals experienced a post-acquisition decline in margins, revenue, and expenses for a two-year period before bouncing back.
In addition, the regulatory environment has tightened, with mergers being increasingly contested by the Federal Trade Commission (FTC), which sees them as curtailing competition, reducing consumer choice, and creating higher managed care prices.
Given the complications of mergers and the increased regulatory scrutiny, AMCs and community provider systems are increasingly turning to partnerships as an alternative to the complexities and increasing risks of an M&A deal. A well-executed partnership arrangement can provide many of the scale advantages of a merger without the regulatory complications—at least so far. Partnership deals are less capital-intensive as a rule (although investment is required) and are easier to take apart if they don’t work.
Brand-name national network affiliations. Such affiliations are offered by national brand-name providers that contractually license their clinical expertise and management services, as well as the selective use of their brand, to grow their referral base and expand access to new market geographies and customer segments. Becoming part of a brand-name network is generally attractive for community hospitals that value their independence and are looking to distinguish themselves in competitive markets. The following are among the best-known examples:
- The Mayo Clinic Care Network, which extends knowledge and specialty expertise through affiliations with community hospitals and physicians both nationally and abroad
- MD Anderson Cancer Center Network Certified Member program in clinical oncology, which provides training for local oncologists, access to MD Anderson specialists, and selective use of the MD Anderson brand
- Cleveland Clinic Specialty Network of Affiliated Hospitals and Alliances, an innovative alliance with community hospitals for cardiovascular and other services providing for the sharing of clinical protocols and management services, in which community hospitals receive the benefits of the clinic’s expertise, participation in shared research projects, and the advantage of the clinic’s brand
The access to specialists at the brand hospitals in the network can be highly beneficial for individual patients, their families, and the “worried well” who want the peace of mind from getting their case reviewed by an outside expert.
Partnerships, alliances, and affiliations short of mergers. AMCs and financially solvent community health systems that have the strength to remain independent have developed a range of partnerships, alliances, and affiliations. Overall, these partnerships between providers and AMCs include alliances with minority equity stakes in acute care systems, shared services collaborations, and accountable care organizations (ACOs) designed for regional or statewide contracting. These types of ACRs have increased substantially in recent years, according to the American Association of Medical Colleges. Generally, outside of densely populated urban markets, the ACRs often are used to develop new approaches to value-based commercial, Medicare, and Medicaid contracts. Partnerships between like-minded AMCs and large community health systems also can improve business performance through supply chain efficiencies, purchasing, and shared technologies.
Joint ventures. Over the past decade, AMCs also have developed various joint ventures with both publicly traded hospital companies and not-for-profit community health systems. These arrangements typically are designed under separate governance structures to acquire and operate community hospital providers ranging from rural hospitals to sophisticated acute care providers. Such joint ventures are challenging because substantial capital investment often is required with the resulting ownership of acute care and ambulatory facilities. Although some of these arrangements proved unsuccessful due to cultural differences (a joint venture between Atlanta-based Emory Healthcare and Nashville, Tenn.-based HCA, for instance), others appear to be standing the test of time and are prospering (Duke LifePoint in Brentwood, Tenn., for example).
In an entirely different series of joint ventures, some community health systems are seeking to move from good to great by creating their own medical schools in new partnerships with universities. According to recent public sources, there are approximately 36 new allopathic medical schools under development or awaiting certification, and since 2010, there have been 18 osteopathic medical schools launched in more than 20 different states. Most of these arrangements will require partnership deals with community health systems to provide the patient base and financial support to be academically viable.
7 Key Success Factors
A fundamental key to success in ACRs appears to be creating a disciplined operating model that supports the strategic goals of both partners over the long term. Analysis of successful ACRs also points to the following seven key factors that must be addressed if an ACR is to realize its potential.
Develop a common vision and realistic goals. To lay the foundation for a successful ACR, it is critical to devote enough time to preliminary conversations. Although simple in concept, defining a common vision, clear goals, and clarity of purpose between two culturally diverse organizations is not necessarily easy in practice. An AMC’s primary goals are to meet its teaching, research, and social/patient care missions—not to run more hospitals. Likewise, community hospitals can be more singularly focused on patient engagement and clinical care. Aligning the two sets of missions and working to develop cultural compatibility between academic and community physicians is a critical first step toward developing consensus on the goals of the relationships.
Emory University’s Blue Ridge Academic Health Group in Atlanta has described this objective as having a “bidirectional” mission, where the community and academic partnership’s goals are both clearly stated and understood to be essential to a partnership’s success.
Focus on product and market synergies first. Collaboration or partnership should begin with a discussion of what the right product—or value proposition—for the market should involve and what resources and skills will be required of the partners to ensure optimum value is delivered for the intended customers. Regardless of how an ACR is to be structured, both the academic and community partners will require an expert, impartial analysis of the market requirements for the clinical venture, including an evaluation of not only the population required to support the combined clinical mission, but also the regulatory environment and likely FTC scrutiny. ACRs can fail for reasons ranging from “too much talking and not enough doing” to “biting off more than they can chew,” so it is prudent to focus on areas of product and market synergies first and develop a shared responsibility for results.
Make sure everyone has “skin in the game.” Transactions involving AMCs and community provider systems are complex. Identifying and gaining support from community physicians and physicians groups is essential—as is understanding and addressing the agendas of powerful department chairs who frequently have research and training agendas of their own. Failure to address issues ofclinical integration and the alignment and governance of faculty practice plans, employed medical staff, and voluntary community medical staff can be the Achilles heel of an ACR. Like any start-up business, ACRs will require investment and nurturing before they pay off. Having a detailed transition plan in place is an essential starting point for integrating key stakeholders and aligning their objectives with the ACR’s strategic rationale.
Establish a governance structure that works for both parties. The balance of governance in an ACR can be especially delicate. AMC physicians are used to having control of their domains, for example, but they cannot assume that their control will extend to their new provider colleagues. Partnerships may offer flexibility in deal structuring that can be advantageous for AMCs that have complicated governance structures and, possibly, university ownership. Meanwhile, the partnership may be of similar value for a community health system that wishes to maintain a degree of independence or avoid being taxed for the extra costs of the academic enterprise. The Duke-LifePoint partnership, for example, has a joint-venture board that oversees the overall partnership and holds the assets of the venture. Some partnerships also have active community boards with medical staff participation. And in some cities, shared governance includes local foundations established with the funds from the hospital purchase.
Ensure both clinical and administrative leadership stay engaged. The governance and operations model should be designed to lock both clinical and administrative leadership into goal-setting and ongoing performance evaluations. Achieving this end requires having an effective organizational structure that provides a voice for faculty and the community medical staff, and an opportunity for them to participate in both clinical and operational decisions. It also may require the development of a dyad organizational management structure that pairs administrative and clinical staff and allows both parties to have meaningful input in key clinical and operations decisions.
Create a sustainable economic business model. Whatever form an ACR might take, involvement in medical education can be costly for the community health system partner. Participation in the academic mission is not for the “faint of wallet.” The cost of academic support payments can in some instances amount to as much as 13 percent of net patient revenues. Economic disconnects can cause partnerships to sour.
Kentucky One, for example, recently terminated its joint operating agreement with the University of Louisville Hospitals following disputes over allegedly insufficient academic support payments and charges of critical cuts in hospital support staffing.
Expect conflict and manage for success. Observed experience in a variety of industries, including health care, suggests that organizational conflicts in complex, collaborative relationships are commonplace. Even the most experienced executive can be surprised by conflict in the ranks, mistakenly assuming that efforts to promote collaboration will develop without organizational tensions. Although differences in opinions and perspectives, competencies, and strategic focus can actually enhance the value of a partnership between an academic and a community health system, both organizations should consider how they might exit the relationship if these tensions were to become unmanageable or if funds flows were to prove insufficient to support the deal. In building an effective ACR, it is wise to accept conflicts as part of the collaborative process and put mechanisms in place for managing disputes at the point of conflict, and for escalating a dispute up the organizational chain of command if necessary. Well-managed conflict can make the organization stronger and ultimately more successful.
A Partnership Driven by Shared Need
AMCs and community health systems have always had a certain level of collaboration, but they historically have existed as two different types of organizations with distinctive cultures. Market pressures have cause this dynamic to shift, creating an environment where AMCs and community health systems need each other more than ever. Not all ACRs are equally functional, and the optimal structure will vary depending on both organizational and market factors. Regardless of the ACR structure being considered, however, any organization contemplating such an arrangement should make sure first to address the seven success factors described here.