





States prioritize workforce initiatives in $25 billion rural grant proposals
But some rural hospitals are expecting an unrealistic financial lift from coming federal grants, said a financial analyst.
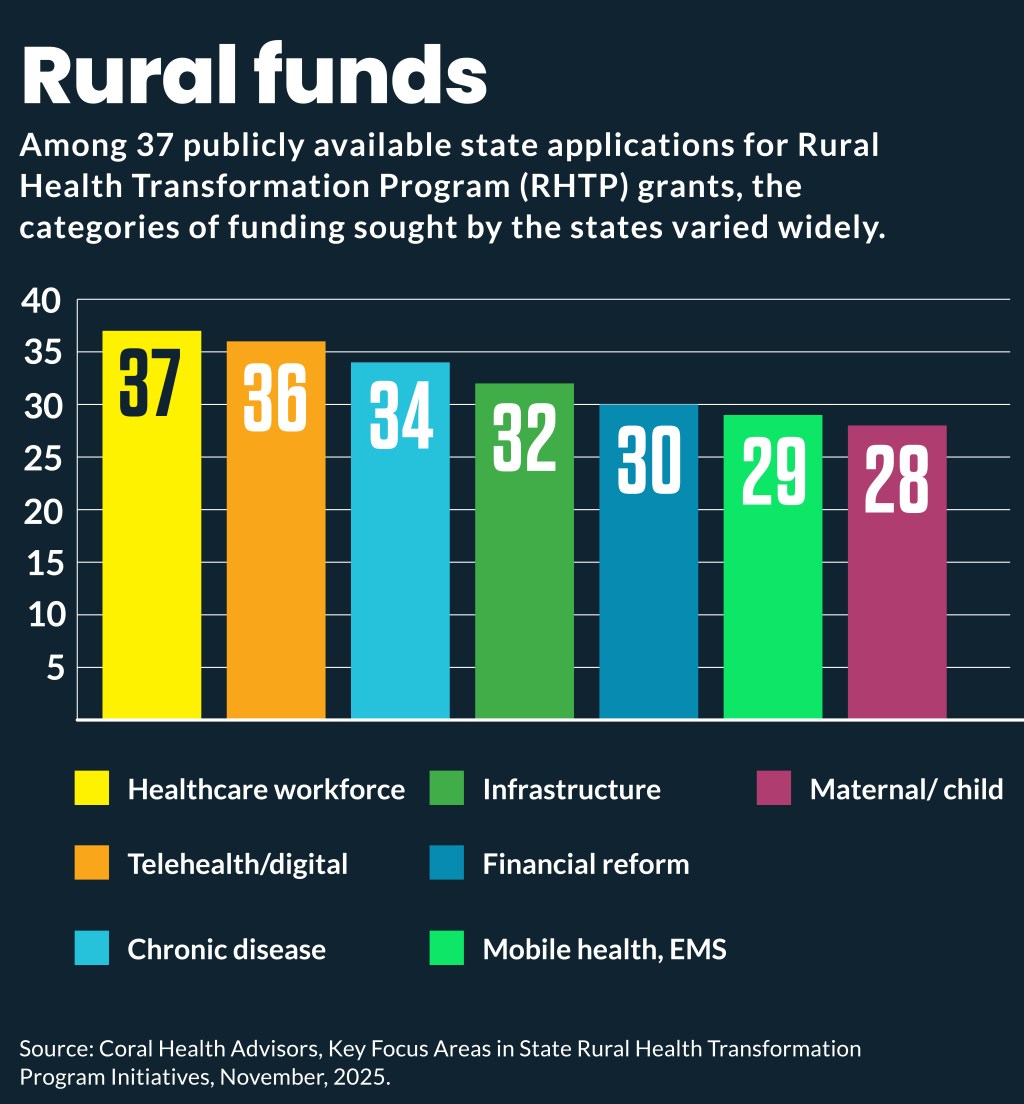
The most common use states are proposing for $25 billion in rural grants from the federal government are for workforce initiatives, according to a recent analysis.
The funding from the One Big Beautiful Bill Act (OBBBA) will provide $50 billion over five years to support rural healthcare. CMS will provide half of those funds to all states whose applications are deemed complete, while CMS will allocate the other half of that money based on specific spending approaches proposed by states in their applications for the cash.
All states submitted their applications for the Rural Health Transformation Program (RHTP) grants by Nov. 5 and CMS plans to announce its decisions on the funding by Dec. 31.
Healthcare workforce initiatives were the only category where funding was requested by every state, according to an analysis of 37 publicly available state grant applications by Coral Health Advisors, which is a consulting firm for health systems and other healthcare entities.
“The focus is shifting from hiring more clinicians to creating new workforce models altogether,” said the analysis.
For instance, Colorado proposed to use $178 million of $1 billion sought to recruit and keep local providers, including physicians, nurses, paramedics and behavioral health professionals, through “streamlined credentialing processes, cross-training and assessing and supporting workforce needs.”
Among the workforce needs it seeks to address is the large percentage of rural counties in the state that lack a practicing OB-GYN, recently 57%.
Other categories of activities that states proposed included:
- 36 states: Telehealth and digital infrastructure
- 34 states: Chronic disease prevention and management
- 32 states: Infrastructure and facility modernization
- 30 states: Payment models, value-based payment, financial reform
- 29 states: Mobile health, emergency medical services
- 28 states: Maternal and child health
“It’s obvious that CMS did a good job with the application process so everybody is sort of onboard to do everything CMS wants — or they are going to try,” said Lynn Barr, founder of Caravan Health. “Getting everybody to move in the same direction was surprising.” She credited that to the way that CMS structured the grant and incentive program.
Data concerns
The biggest concern that the state applications raised for Barr was the push of many of them to expand health information exchanges (HIEs) as a way to boost and track performance on costs and quality.
“The [HIEs] don’t really have data; they’re just like post offices,” Barr said. “So, it’s not a robust and reliable source of data.”
For example, New Mexico proposed to use $53 million for various data projects, including incentivizing the use of its HIE. The state aims to increase provider participation in the HIE by 30%.
The best options among these are states have requested funds to build “community HIEs,” which are actually data warehouses that could improve access to needed data, she said.
North Dakota
North Dakota’s approach stood out to Barr since it planned to use RHTP funds to launch an all-payer claims database and outcomes measurement tool.
The state aims to use those “to enhance transparency and accountability in pricing for consumers while helping North Dakota better evaluate cost, quality, and differences across systems,” according to its application.
That kind of approach could help address the problem of poor data, which stymies efforts to improve quality and lower costs in the healthcare system, Barr said.
Hospitals’ view
Mark Pascaris, senior director for Fitch Ratings, warned in a recent interview that some hospitals may be expecting too much benefit from the rural funds as they brace for $1 trillion in nationwide healthcare cuts from the OBBBA.
“There are some organizations that are a little too optimistic about the rural health fund,” Pascaris said. “For some specific hospitals, in some specific markets, in some particular states, it actually will be a net benefit to them, maybe even outweighing Medicaid cuts.”
But for the overall hospital industry, the $50 billion in rural funds will be a “drop in the bucket” compared to the law’s $1 trillion in cuts, he said.
It also remains unclear which hospitals will benefit from those funds, as illustrated by the push of urban academic medical centers for rural funding since they receive many referred rural patients.