Payment Models
What to expect from an inpatient-outpatient site-neutral payment system for Medicare
An analysis shows that moving Medicare inpatient and outpatient payments for procedures to a site-neutral payment system will reduce Medicare expenditures, but such a move presents challenges, including defining exceptions and ensuring patient safety.
Published
December 23, 2025
3:10 pm
|
Updated
January 29, 2026
8:35 am
A recent final rule for the Medicare outpatient prospective payment system (OPPS) gradually eliminates over a three-year period the requirement that some procedures can only be performed in an inpatient site of service.a In the rule, CMS eliminates what is colloquially known as the “inpatient-only list” to make more procedures eligible to be performed in a hospital outpatient department (HOPD). This is a first step toward establishing a hospital site-neutral inpatient-outpatient (SNIO) payment system for a wide range of procedures.
The ramifications of this change, discussed here, underscore the need for hospitals and health systems to plan for the implementation of an SNIO payment system. Foremost among these considerations will be the need to address patient safety concerns associated with such a change.
Regulatory momentum toward SNIO payment
With the Medicare hospital insurance trust fund (Part A) projected to become insolvent in 2033 and hospital prices increasing at triple the rate of inflation, Medicare payment reforms that constrain hospital Medicare expenditures seem inevitable.b Senators Bill Cassidy (R-LA) and Maggie Hassan (D-NH) recently proposed a bipartisan framework for a site neutral (SN) payment system, which defined site neutral services as those services where “the same care can be safely provided in different settings.”c Under an SN payment policy, Medicare would pay the same rate for the same service, regardless of where the service is delivered.
To date, SN reform proposals have focused on SN payments involving HOPDs, ambulatory surgery centers and physician offices.d However, equalizing payment for equivalent inpatient and outpatient procedures creates a strong incentive for hospitals to shift more services to the lower-cost HOPD setting, potentially resulting in a substantial reduction in Medicare hospital expenditures.
Patient safety is an important consideration in such a shift. To ensure that an SNIO payment system for procedures meets the requirements in the Cassidy-Hassan proposal, there must be clear operational definitions of what constitutes same care and safely provided. The wide range of inpatient severity of illness means that determining which inpatients can have a procedure performed safely in a HOPD is not just a question of the procedure being performed but, more important, the clinical condition of the patient. Thus, patient safety is a critical concern that must be addressed in an aggressive expansion of procedures that can be performed in an HOPD. It is essential that a hospital SNIO payment system have explicit criteria that identifies those inpatients who can safely have a procedure performed in such a setting. (See the sidebar below, “Criteria for patients who cannot safely undergo an SN procedure in an HOPD,” for a description of the requisite criteria.)
To assess the impacts of a move to SNIO payment, we used Medicare claims data to determine the difference in inpatient and outpatient payment for 27 categories of procedures and estimated the financial impact and bed-day impact of the new payment system.
Basic structure of an SNIO payment system
Under the SNIO payment system, each inpatient would be evaluated at discharge to determine whether the hospital should be paid the standard inpatient payment rate or an SNIO payment rate for the equivalent procedure performed in an HOPD. Operationally, each patient would be evaluated at discharge to determine:
- Whether the patient had a procedure that qualifies for SN payment
- Whether the SN procedure can be safely performed in an HOPD based on the clinical condition of the patient
- The applicable SNIO payment rate for the SN procedure
Determining whether a hospital is paid the SNIO payment rate is a process that can be fully automated using SN grouper software, similar to the grouping assignment software that CMS makes available to hospitals in the current inpatient and outpatient payment systems. Hospitals can integrate the SN grouper with their post-discharge billing systems, thereby minimizing the operational impact.
Determining the subset of procedures included in an SNIO payment system
The Medicare inpatient prospective payment system (IPPS) pays hospitals using Medicare severity diagnosis-related groups (MS-DRGs).e In MS-DRGs, low resource-intensity procedures such as colonoscopies do not impact the MS-DRG assignment and payment. Procedures with higher resource intensity such as cholecystectomy (referred to as operating room [OR] procedures) impact MS-DRG assignment and payment. The subset of procedures eligible to be included in an SNIO payment system are the OR procedures as defined in MS-DRGs.
Again, however, criteria also must be considered to address concerns about patient safety when determining whether a patient should undergo an SNIO-payment-eligible procedure in an HOPD.
SNIO payment rates
To compute the equivalent OPPS payment rate for an SN procedure, the SNIO grouper must also be applied to the outpatient data. The SNIO payment rate for an SN procedure would be based on the OPPS payment rate for the subset of outpatients with an equivalent SN procedure. Identifying equivalent inpatient and outpatient procedures is challenging due to the coding differences between inpatient procedures and procedures in the HOPD, which involve the use of the International Classification of Diseases, 10th revision, Procedure Coding System (ICD-10-PCS) versus the Current Procedural Terminology (CPT) coding system, respectively.f
For example, under ICD-10-PCS, a percutaneous transluminal coronary angioplasty (PTCA) includes the insertion of a stent as part of a single code, whereas under the CPT system, stent insertion is assigned as a separate code. To identify equivalent outpatient PTCA patients, the SNIO grouper must recognize that the two outpatient CPT procedure codes are not clinically distinct but represent a single procedure, which means for outpatients both the codes should be included in determining the SNIO payment rate for a PTCA. Identifying equivalent ICD-10-PCS and CPT procedure is a process that is performed by CMS to determine the SNIO payment rate from the OPPS data. Operationally, the SNIO grouper requires only the inpatient ICD-10-PCS codes, so hospitals do not have to deal with the challenges of aligning ICD-10-PCS and CPT data.
The SNIO payment rate can be determined in multiple ways using the existing OPPS payment rates. For example, the SNIO payment rate could be set based on a blending of the IPPS and OPPS payment rates for an SN procedure. In the following analysis, the SNIO payment rate was set as the average OPPS payment for each SN procedure, which provides an estimate of the maximum SNIO payment impact. Any form of blending of the IPPS and OPPS payment rates would reduce the estimated SNIO payment impact.
Analysis of the SNIO payment impact
We used the pre-pandemic calendar year 2019 Medicare Standard Analytic Files (Limited Data Set) containing 100% of Medicare fee-for-service inpatient and outpatient claims to analyze the impact of an SNIO payment system.g Only hospitals paid under the Medicare IPPS and located in the 50 states and the District of Columbia were included. As noted previously, 27 categories of relatively high-volume procedures routinely performed on an inpatient basis or in an HOPD were selected for the analysis (see the list at the end of this article). A prototype SNIO grouper was developed and used to determine which patients were eligible to have the SN procedure performed in an HOPD.
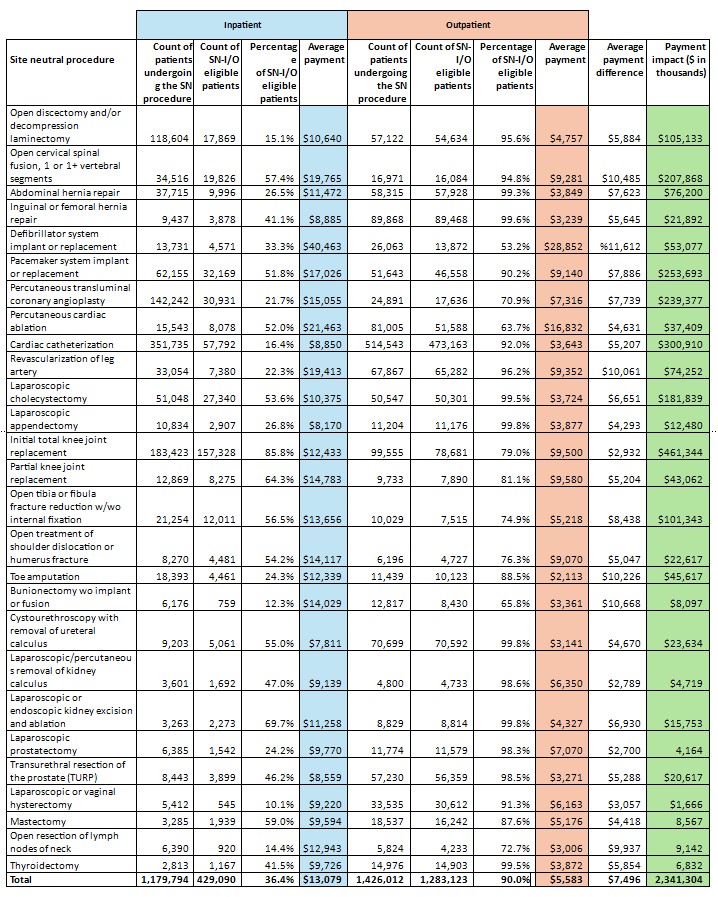
The exhibit below shows that, of 1,179,794 inpatients undergoing any of the 27 procedures, 429,090 (36.4%) were eligible to have the procedure performed in an HOPD. The average actual Medicare IPPS payment across the 27 SN procedures for SNIO eligible inpatients was $13,079. Meanwhile, among 1,426,012 outpatients undergoing any of the 27 procedures, 1,283,123 (90.0%) could be included in the determination of the average OPPS payment.
Site neutral inpatient and outpatient (SNIO) volume and payment differences
| Site | Number of patients undergoing the SN procedure | Count of SNIO eligible patients | Percentage of SNIO eligible patients | Average |
|---|---|---|---|---|
| Inpatient | 1,179,794 | 429,090 | 36.4% | $13,079 |
| Outpatient | 1,426,012 | 1,283,123 | 90.0% | $5,583 |
The main clinical reason for the exclusion of some outpatients was the presence of multiple distinct procedures. The average actual Medicare OPPS payment across the 27 SN procedures was $5,583. The average payment difference between IPPS and OPPS payments across the 27 SN procedures was $7,496, which ranged from $11,612 for defibrillator implants to $2,700 for a laparoscopic prostatectomy.
The payment impact of an SNIO payment system is the sum of the product of the average payment difference between IPPS and OPPS payments for each SN procedure and the number of inpatients who are eligible to have that SN procedure performed in an HOPD. Across the 27 SN procedures, the payment impact of an SNIO payment system is $2.34 billion. The payment impact ranged from $461.3 million for total knee replacement to $1.7 million for laparoscopic vaginal hysterectomy. (See the exhibit below showing results of all 27 SN procedures.) The likely expansion of the number of procedures included in a SNIO payment system beyond the 27 SN procedures will significantly increase the estimated payment impact.
This analysis assumed that the SNIO payment for inpatients with an eligible SN procedure would be the average OPPS payment for the SN procedure, paid to the hospital as a single fixed payment that is payment in full. However, the SNIO payment rates of individual hospitals would be adjusted using either the IPPS or OPPS standard payment adjustments (e.g., based on the wage index). The SNIO payment could be covered under either Medicare Part A or Part B. From the Medicare beneficiary’s perspective, coverage under Part A would avoid the copayments in Part B. Such operational design issues would need to be decided before any broad SNIO payment system is implemented.
Shifting more procedures to the outpatient setting will also free up more bed capacity. Bed shortages and overcrowded emergency departments are becoming common in some geographic areas.h Assuming an 85% occupancy rate, the shift of 429,090 patients from inpatient to the HOPD would free up 1,170,063 bed days (on average 2.673 days per inpatient), equivalent to increasing hospital bed capacity in the U.S. by 3,771 beds.
Safety concerns are front and center
Implementation of a SNIO payment system will reduce Medicare hospital expenditures, but the patient safety concerns it raises cannot be ignored. The regulations implementing a SNIO payment system should describe:
- Clear operational criteria that identify those inpatients who can have an SN procedure safely performed in an HOPD
- The specific methodology used to determine SNIO payment rates from the OPPS payment rates
- Any payment adjustments to the SNIO payment rates for all legitimate reasons for variation in SN procedure cost among hospitals.
Most important, hospitals should plan for the potential implementation of a SNIO payment system and be actively engaged during the regulatory comment period of any CMS proposed rules for implementing a SNIO payment system. In particular, hospitals should comment on the subset of procedures proposed for inclusion in a SNIO payment system.
Footnotes
a. CMS, “Calendar year 2026 hospital outpatient prospective payment system (OPPS) and ambulatory surgical center final rule (CMS-1834-FC),” fact sheet, Nov. 25, 2025.
b. Guidi, T.U., “Medicare’s hospital outpatient prospective payment system: OPPS 101 (part 1 of 2),” Journal of Oncology Practice,” November 2010; and Committee for a Responsible Federal Budget, “Analysis of the 2025 Medicare Trustees’ Report.” June 18, 2025.
c. Office of Sen. Bill Cassidy, MD. “Cassidy, Hassan release policy framework on Medicare site-neutral reform to lower health care costs,” press release, Nov. 1, 2024.
d. Albanese, J., “Opportunities for Medicare site neutrality in 2025,” Paragon Health Institute. Jan.8, 2025.
e. CMS, “Inpatient prospective payment system (IPPS),” page last modified Sept. 10, 2024.
f. CMS, “ICD-10-PCS official guidelines for coding and reporting,” 2020, Sept. 10, 2024; and American Medical Association, “CPT overview and code approval,” updated Nov. 21, 2025.
g. CMS.gov, “Standard Analytical Files (Medicare Claims) – LDS,” updated Aug. 21, 2025.
h. McGrath, C., and Niezgoda, A., “Amid capacity crisis, Massachusetts General Hospital asks state for more beds to ease waits,” NBC Boston 10, Jan. 19, 2024.
Criteria for patients who cannot safely undergo an SN procedure in an HOPD
An operational SNIO payment system must establish criteria that explicitly define the concept of safely provided. Inpatients who undergo an SN procedure and meet any of the following criteria should not be considered eligible for the SN procedure performed in a hospital outpatient department (HOPD).
The reason for admission is inherently complex. The reason a patient is admitted to the hospital can be inherently complex with a high risk of morbidity or mortality, or because the procedure requires sophisticated technology (e.g., a bone marrow transplant). For example, a percutaneous transluminal coronary angioplasty (PTCA) can be performed as an inpatient procedure or in an HOPD. A patient who is admitted to a hospital for a myocardial infarction (heart attack) and undergoes a PTCA, however, is inherently complex and would not be eligible to have the PTCA performed in an HOPD.
The procedure is clinically inconsistent with the reason for hospital admission. A patient’s admission to the hospital should be consistent from a clinical standpoint with the procedure performed. A male patient admitted for pneumonia who develops urinary retention and requires a prostatectomy would not be considered eligible for the prostatectomy to be performed in an HOPD. There are specific MS-DRGs for patients undergoing procedures that are clinically inconsistent with the reason for hospital admission — i.e., MS-DRGs 981-983 (Extensive OR procedures unrelated to the principal diagnosis) and 987-989 (Non-extensive OR procedures unrelated to the principal diagnosis).
The patient has a high severity of illness at the time of admission. A patient with a high severity of illness at admission increases surgical risk and should not be considered eligible for an SN procedure performed in an HOPD. The IPPS identifies patients with major complications or comorbidities, which in turn can be used to identify high severity of illness at the time of admission.
The patient has multiple clinically distinct procedures.In general, when a patient is scheduled for an HOPD procedure, the HOPD visit is explicitly for that single procedure. Inpatients are more likely to undergo multiple clinically distinct procedures during their hospital stay (e.g., cardiac catheterization and revascularization of leg artery), in which case they would not be considered eligible to undergo an SN procedure in an HOPD.
In short, for any patient not considered eligible to have an SN procedure performed in an HOPD, the hospital would be paid the IPPS payment.
27 categories of relatively high-volume procedures routinely performed on an inpatient basis or in an HOPD
- Open discectomy and/or decompression laminectomy
- Open tibia or fibula fracture reduction with/without internal fixation
- Open cervical spinal fusion, one or more vertebral segments
- Open treatment of shoulder dislocation or humerus fracture
- Abdominal hernia repair
- Toe amputation
- Inguinal or femoral hernia repair
- Bunionectomy without implant or fusion
- Defibrillator system implant or replacement
- Cystourethroscopy with removal of ureteral calculus
- Pacemaker system implant or replacement
- Laparoscopic/percutaneous removal of kidney calculus
- Percutaneous transluminal coronary angioplasty
- Laparoscopic or endoscopic kidney excision and ablation
- Percutaneous cardiac ablation
- Laparoscopic prostatectomy
- Cardiac catheterization
- Transurethral resection of the prostate
- Revascularization of leg artery
- Laparoscopic or vaginal hysterectomy
- Laparoscopic cholecystectomy
- Mastectomy
- Laparoscopic appendectomy
- Open resection of lymph nodes of neck
- Initial total knee joint replacement
- Thyroidectomy
- Partial knee joint replacement
Site neutral volume and payment differences for 27 high-volume procedures