





Fast Finance
Finances drive REH conversion
Conversion drove operating margin improvement from worse than -20% to 2%.
Published
March 10, 2026
8:25 am
One hospital’s conversion to a rural emergency hospital (REH) has reversed its financial challenges and allowed service changes sought by the local community.
Negative operating margins were the norm for Mercy Hospital in Moundridge, Kansas, for more than 10 years before it considered a major strategic shift.
The 15-bed prospective payment system rural hospital came out of the COVID-19 pandemic facing spiraling costs, which were outstripping revenue and showing no sign of abating. It had no cash reserves, faced significant staff turnover, owed more than $2 million to vendors and lacked a capital improvement budget.
“We’ve got aging accounts payable, we can’t pay our bills, we can hardly make payroll. And now, how are we going to get out of this hole?” Aaron Herbel, administrator and CFO of Mercy Hospital, recalled thinking at the time.
That’s when Congress authorized REHs, which offer a monthly facility payment (over $3.4 million annually in 2025) and 105% of the hospital Outpatient Prospective Payment System (OPPS) rate. In exchange, hospitals would need to drop inpatient care and provide around-the-clock emergency department (ED) services.
Mercy undertook the conversion on Jan. 1, 2024, halfway through its fiscal year.
The change resulted in improving operating margins from worse than -20% in both FY22 and FY23 to -6% in FY 24 and 2% in FY25.
“That’s the first time outside of COVID relief funds that we’ve had a profit in over 10 years as an organization,” Herbel said.
Options considered
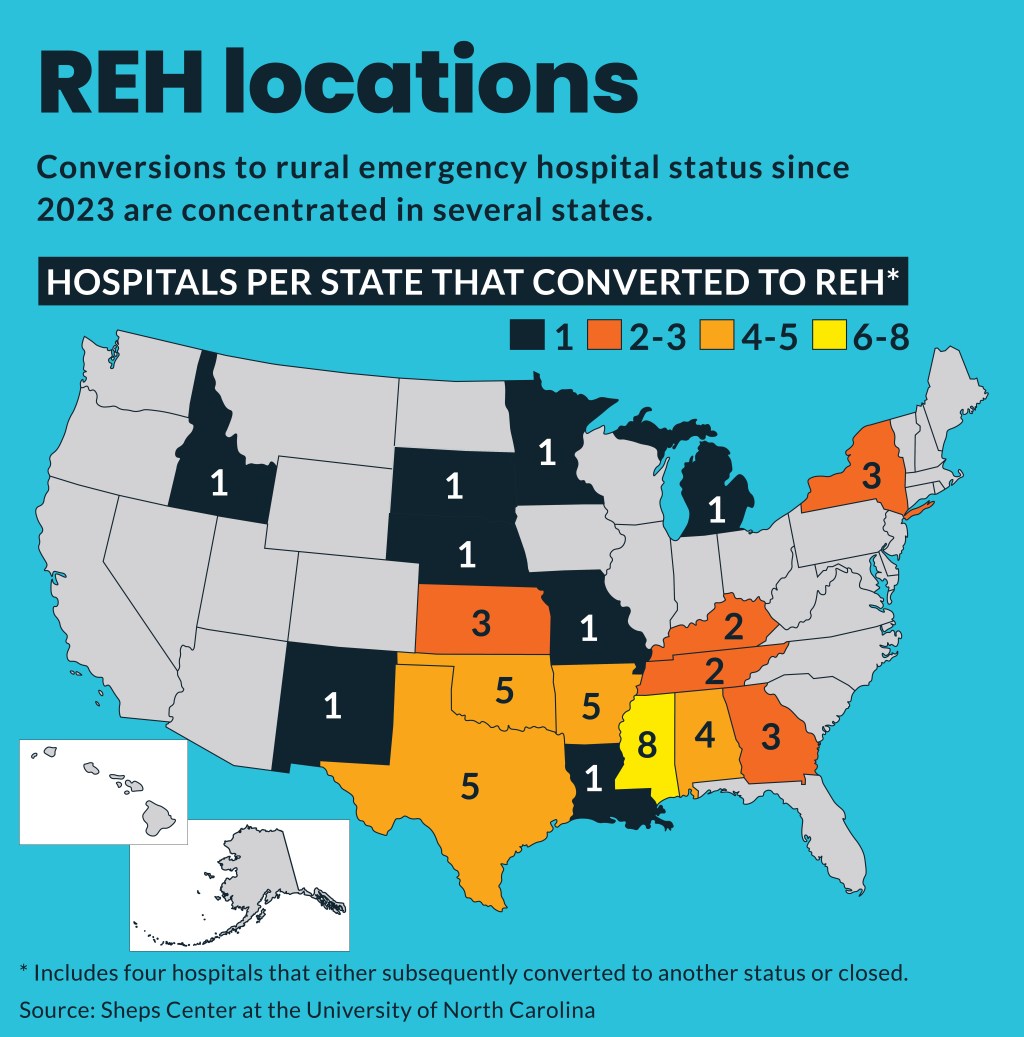
As of November 2025, 44 hospitals have converted to REH status, according to tracking by the Sheps Center at the University of North Carolina at Chapel Hill.
But Mercy considered other options before it changed to REH status. A common option some rural hospitals used to improve their finances was conversion to a critical access hospital (CAH). However, Mercy was ineligible because it was inside the 35-mile minimum distance to another hospital, which CMS enforces for CAH designation.
The hospital also considered a sale to a health system, but leaders were concerned that it would run contrary to its founding mission as a service opportunity for the local Mennonite community.
“The board felt like our mission wasn’t complete yet,” said Herbel. “While they considered a sale, we felt if there was a way to move forward and keep the hospital open in the community as a project to the church, they wanted to do that.”
Why it fit
Giving up inpatient services, as required by the REH designation, tracked with patient trends at the facility.
When Herbel started at Mercy in 2017, about 60% of its net patient revenue was inpatient; but by FY24, it was only about 35%.
The cost trend also was a critical concern. From 2019 to 2022, net inpatient revenue grew about 12.5% while expenses increased by about 38%.
“What contributed to the large negative operating margins in 2022 and 2023 was that we had added staff and equipment, and we did things to expand our services,” Herbel said. “And we did grow our volume, but the cost just outran that revenue increase.”
The conversion allowed the hospital to reduce its staff but use the savings to increase salaries. Herbel credited that move with cutting turnover from 21% in 2022 to 7% in 2025.
Beyond finances, the status change allowed the hospital to match the needs identified by the local community, who Mercy broadly surveyed before it undertook the conversion. In response to the survey results, the post-conversion hospital added a walk-in clinic with weekend hours.
“The walk-in clinic was the No. 1 requested service,” Herbel said. “We’d asked them, and that’s what they said and that made it easy for us to move forward with confidence because we knew that’s something the community wanted from us.”
It also grew its outpatient IV infusion therapy services and continued services such as outpatient lab and radiology services, colonoscopies and outpatient surgical procedures.
“That really allowed us to expand the demographic of patients that we’re caring for,” Herbel said. “We’re seeing a lot of new people come into our facility that historically weren’t patients of our organization.”
As a result, patient volumes for its ED and walk-in clinic now exceed those Mercy previously had in its ED. Additionally, the acuity of its ED patients has increased with more Level V ED visits in 2025 than in the year before.
“We can still take care of those stroke and STEMI patients when they walk in the door,” Herbel said. “And then we’re able to give them immediate lifesaving intervention and facilitate that transfer to whatever they’re needing, whether it’s surgical or inpatient hospital placement.”
Buy-in was key
After Congress authorized the REH model in 2020, the board chair authorized Herbel to investigate its potential fit. After the board consideration, the idea was presented in public forums to gather the community’s perspective.
“We presented the REH option as a positive way to move the community forward and sustain healthcare in the community by demonstrating with actual data the number of patients that we were going to be able to continue to care for,” Herbel said. “And showing how converting to an REH was going to stabilize the hospital’s operational profit and loss [both of which] would allow us to make the necessary improvements and capital updates to continue providing care in this community for years to come.”
When a member of the community asked what the hospital’s physicians thought of the REH, Mercy’s medical director explained that after evaluation, the physicians thought it was the best option.
“When the physician said that, the questions from the community stopped,” Herbel said. “They’re like, ‘If the doctors think this is the best thing to do, then we can get behind it also.’”
Mindset shift
Herbel sees the REH conversion as just the latest way Mercy is trying to meet its vision statement to be “the best small hospital in Kansas.”
Key to that was embracing the idea that it would not try to outcompete other hospitals in the region, which offer services like ICUs, inpatient surgery and obstetric departments.
“Rural communities need to embrace the concept that they need to be what their community needs them to be and not try to be everything for everybody” Herbel said. “Because the current cost and expense structure within the health hospital space doesn’t allow for the small, critical access hospitals to offer 18 subspecialties.”
Herbel said he has heard from CEOs of other rural hospitals that converted to REH status and they said it also improved their organizations’ finances.
The REH model also has benefited neighboring PPS hospitals, Herbel said, since those in his area have seen increases in patient volumes through the patients Mercy sends to them.
“That’s helping their bottom line because it’s another patient they’re able to care for within their capacity, and it helps them financially by sharing services in that way,” Herbel said.