





Fast Finance
Minnesota hospitals: 340B revenue from drugmaker profits
At least five states are considering bills seeking more insight into 340B program activities.
Published
March 10, 2026
8:21 am
The $1.3 billion Minnesota providers garnered in 2024 from the 340B program was money that would have gone to drugmaker profits, states the hospital group.
The latest state-mandated report on Minnesota covered entities’ earnings from 340B found:
- $1.34 billion in net 340B revenue
- Increase from $630 million net revenue in 2023
- Likely an undercount due to missing some office-administered drugs
The increase from 2023 to 2024 primarily stemmed from the latest report adding office-administered drugs by covered entities, according to the state report. Net revenue came from subtracting the 340B drugs’ $1.53 billion acquisition costs and $165 million administrative costs from their $3.04 billion reimbursements.
“Without 340B, these funds would flow to pharmaceutical company profits, increasing the likelihood that taxpayers will have to spend more to provide health care for low-income Minnesotans,” according to a Minnesota Hospital Association (MHA) emailed statement.
Although the report does not delve into how providers use 340B funds, MHA officials said they are used to improve health in communities, including keeping rural emergency departments open.
“Most importantly, 340B helps offset chronic underpayment in public programs,” MHA stated.
MHA said Medicare and Medicaid typically reimburse hospitals for the cost of care at less than 80 cents on the dollar. And nearly 60% of patients in Minnesota hospitals are covered by those programs.
Despite the 340B revenue, 2024 hospital losses “resulted in an unprecedented series of service-line contractions in 2025, like closures of labor and delivery services across the state,” stated MHA.
Key findings
The report’s covered entity net revenue findings included:
- $1.08 billion for disproportionate share hospitals (DSH)
- $135 million for critical access hospitals (CAH)
- $92 million for other hospitals
- $22 million disease-specific federal grantees
- $8 million safety net federal grantees
The new requirement for Minnesota covered entities to report 340B revenue from administered drugs is not always straightforward because of hospitals’ “buy-and-bill” strategy, [which] complicates reporting, said Sayeh Nikpay, PhD, a 340B researcher at the University of Minnesota School of Public Health.
“However, they are likely going to have to get used to it as administered drugs are a big part of the overall picture,” Nikpay said.
The report also detailed $165 million in total operational costs for 340B covered entities. That broke down to:
- $120 million for contract pharmacy
- $17 million for other external costs
- $28 million for internal administrative costs
The report also found a wide range of total operational costs as a percentage of gross 340B revenue. Operational costs for the top 10% of all hospital types ranged from 13% for other hospitals to 42% for CAHs. Whereas the top 10% of grantees had total operational costs of 60% or greater of their gross 340B revenue.
Those administrative costs may increase after some manufacturers recently further ramped up claims data submission requirements on covered entities.
“So, it’s a new reality that likely hospitals will have to get used to,” Nikpay said.
Those expanded data submission requirements followed the Trump administration’s February withdrawal of a 340B rebate pilot.
Wider trend
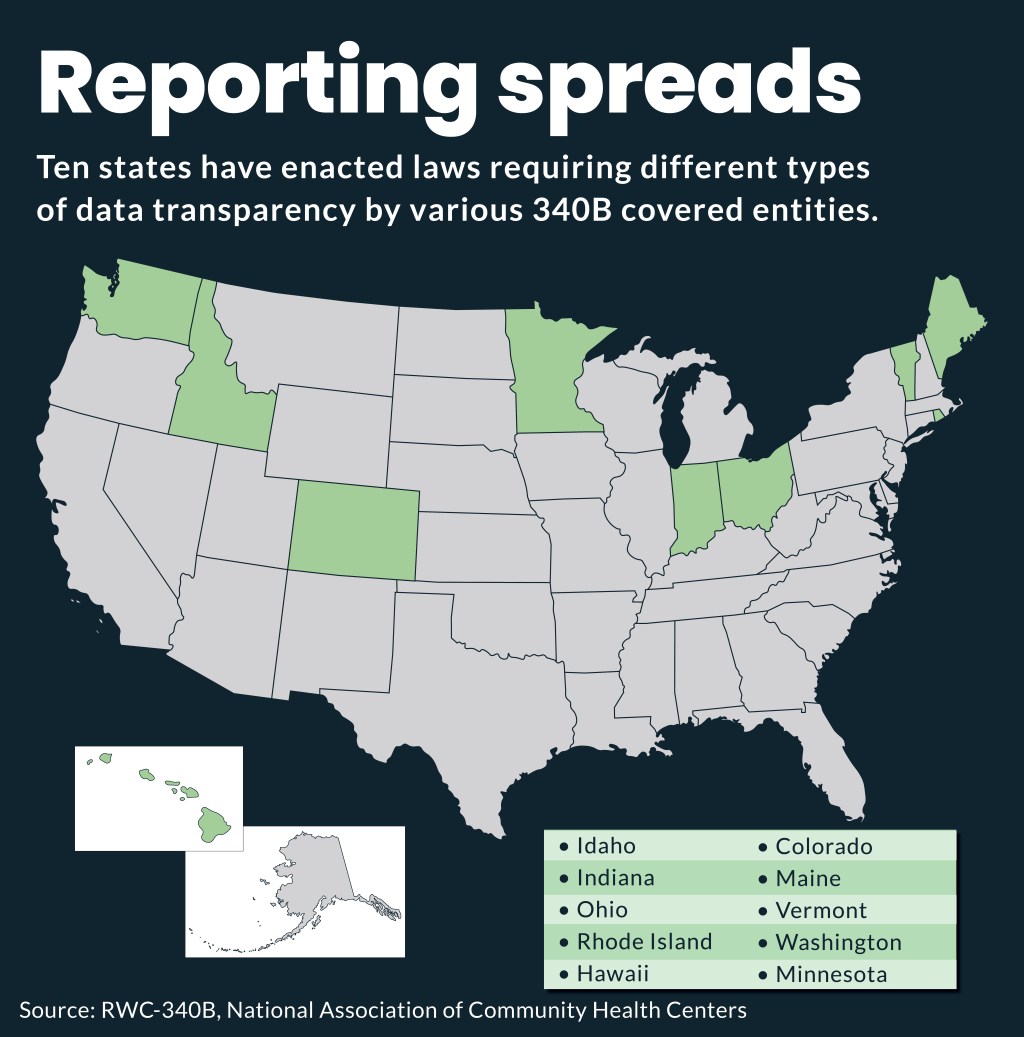
Minnesota is one of 13 states that have passed 340B transparency legislation or are issuing a report on 340B, according to the 340B covered entity report to the Minnesota legislature. However, there is wide variation among state requirements on timing, data and other details.
Minnesota was the first to report 340B provider revenue data publicly last year.
Idaho enacted similar reporting requirements in 2025 and so far this year, at least five states are considering bills seeking more insight into 340B program activities, according to a recent update by the National Conference of State Legislatures.
Broader push
The latest Minnesota report also may fuel the push by some to overhaul the 340B program.
For instance, the finding that 45% of providers’ net 340B revenue, or $608 million, came from commercial reimbursement was cited by Shawn Gremminger, president and CEO of the National Alliance of Healthcare Purchaser Coalitions (NAHPC).
“While the ever-expanding size of the program is old news, they were able to quantify something else that should make employers and purchasers sit up straighter: Employers are funding nearly half of the 340B ‘spread’ in Minnesota, he said in a LinkedIn post. “If you represent employers, unions or working families, it’s hard to read that and not ask: ‘Where is that money going, and what are purchasers getting for it?’”
NAHPC is among employer groups that have begun to push for an overhaul of 340B because they say it is adding to employers’ insurance costs.
Providers dispute that assertion and say health insurance costs are driven by pharmaceutical pricing practices, administrative complexity and broader market dynamics.