





Fast Finance
Payer study: AI coding drives a multibillion-dollar spending increase
A provider expert argues the increase reflects improved documentation accuracy rather than upcoding.
Published
March 17, 2026
8:17 am
After years of allegations by payers that the increasing hospital adoption of AI-driven billing is increasing costs, the industry has produced the first research that allegedly quantifies it.
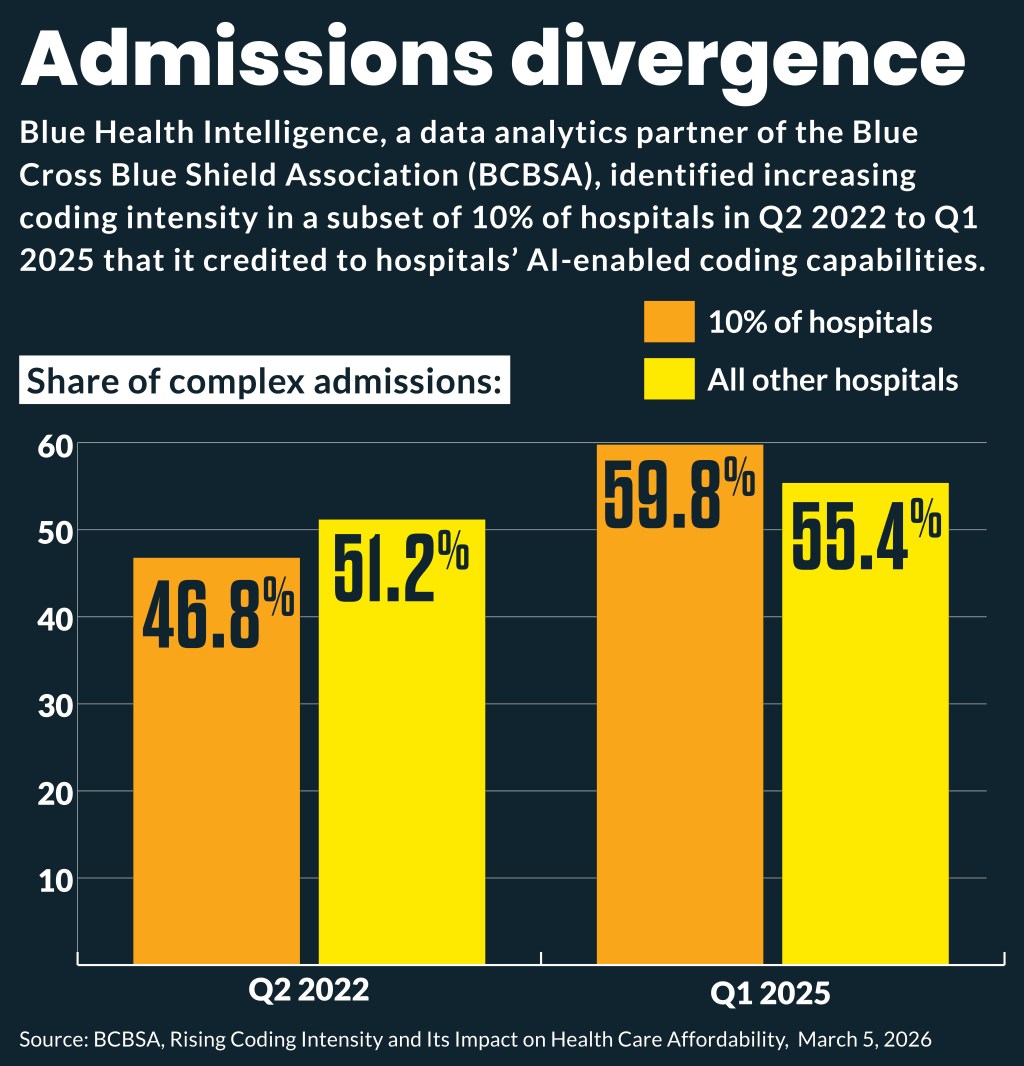
Hospitals’ AI-enabled coding capabilities drove $2.3 billion in increased spending in a recent three-year period, according to new research from Blue Health Intelligence, a data analytics partner of the Blue Cross Blue Shield Association (BCBSA). That broke down to:
- An estimated $663 million in increased inpatient spending
- At least $1.67 billion in increased outpatient spending
The estimates stemmed from a Q2 2022 to Q1 2025 analysis of commercial claims data for hospitals paid through a member plan.
It found that 10% of the hospitals, which generally had a lower share of complex-coded admissions, had a larger increase in inpatient admissions coded as complex than the other 90% of hospitals. That 10% saw complex-coded admissions increase by 13.1 percentage points to 59.8%. The remaining 90% of hospitals had a 4.2 percentage point increase of inpatient admissions coded as complex over this three-year period.
“The variation seen between the 10% of hospitals showing high growth relative to the rest suggests that there is something happening in these hospitals to drive substantial changes in a short period of time,” wrote the authors.
Shawn Stack, director of perspectives and analysis at HFMA, said the study appears to conflate improved documentation accuracy with “aggressive coding.”
Over the past decade, hospitals have made substantial investments in clinical documentation improvement (CDI) programs to ensure that medical records accurately reflect patient conditions and severity of illness, he said. And many AI-supported tools used by hospitals assist clinicians in identifying conditions already present in the medical record but historically under-documented or inconsistently coded.
“Capturing these diagnoses more accurately does not necessarily represent upcoding — in many cases, it reflects better clinical documentation and data integrity, which is very important in value based care [VBC] and clinical outcome analysis,” Stack said.
OB example
The BCBSA study delved into maternity admissions, which emerged as an area where reported complexity significantly increased; in particular, admissions increased that were coded with acute posthemorrhagic anemia.
Among the high-growth hospitals, maternity admissions being coded with postpartum anemia increased from 4% in Q2 2022 to 12.3% by Q1 2025. Low-growth hospitals saw a small increase — 7.9% in Q2 2022 to 8.2% by Q1 2025.
The conclusion that higher-acuit coding was not associated with increased care came from the finding that rates of transfusion, common in cases of acute posthemorrhagic anemia, remained relatively flat.
The finding suggested to the authors “a discordance between the reported level of complexity of the patient and the treated condition.”
However, Stack said the study’s premise that clinical validity requires that specific interventions must always accompany given diagnoses, such as a blood transfusion accompanying acute posthemorrhagic anemia, is not supported by clinical practice.
“Many cases of postpartum anemia are managed conservatively, including through monitoring, iron therapy, medication or observation, particularly when transfusion thresholds are not met,” Stack said. “The absence of a transfusion does not invalidate the diagnosis.”
Another finding
A separate, recent study by Trilliant Health, which advises providers, payers and drugmakers, used national all-payer claims data to examine evaluation and management (E/M) billing patterns at six large hospitals and health systems from 2018 to 2024. The hospitals and health systems were selected because they publicly announced adoption of ambient AI scribing systems.
It found that established and new patient visits shifted toward higher-intensity E/M codes across those health systems, although to differing degrees.
Among established patient visits with high-intensity E/M code, the largest increases across all ICD-10 diagnosis chapters were in:
- Factors influencing health status
- Mental and behavioral disorders
- Neoplasms
- Blood and immune disorders
- Digestive diseases
Fraud allegations
AI billing is the most prevalent nonclinical use of the new technology, Hannah Neprash, an associate professor at the University of Minnesota’s School of Public Health, said at a March 11 VBC conference.
“And the challenge is really knowing whether coding increases reflect truly more complex care that’s happening or just higher spending for them for the same stuff. It’s probably somewhere in between,” Neprash said. “Payers increasingly believe the latter, and they’re pursuing these down-coding strategies, which is why I call this the AI coding wars, because it’s kind of a one-upsmanship approach.”
The Trilliant authors noted that much of the AI underlying the hospital and health systems’ clinical documentation and coding systems, especially natural language processing and large language models, are rules driven. Because of that, the increase in coding intensity “could reflect that individual providers have historically under-coded, either out of incomplete clinical documentation, suboptimal coding practices, fear of violating the False Claims Act or some combination thereof,” they wrote.
The authors noted that payers implying fraudulent provider billing from AI-enabled coding platforms have the evidence from detailed AI scribing to audit the accuracy of the claim.
“Within this context, the increase in coding intensity found in this study is unlikely attributable to provider fraud,” the authors wrote. “For the observed increase in coding to be fraudulent would require some amount of conspiratorial activity, either between AI-enabled tool providers or physicians across unrelated health systems.”