





Financial Sustainability
Rural hospitals seeing signs of financial hope
Recent reports of improving finances among the nation’s rural hospitals may be a beacon for the many that continue to face severe financial challenges.
Published
March 30, 2026
4:08 pm
|
Updated
March 31, 2026
4:10 pm
After years of struggling with financially precarious positions, rural hospitals saw their overall finances begin to improve in 2025. Both individual hospital strategies and external payment changes could determine whether that trend continues.

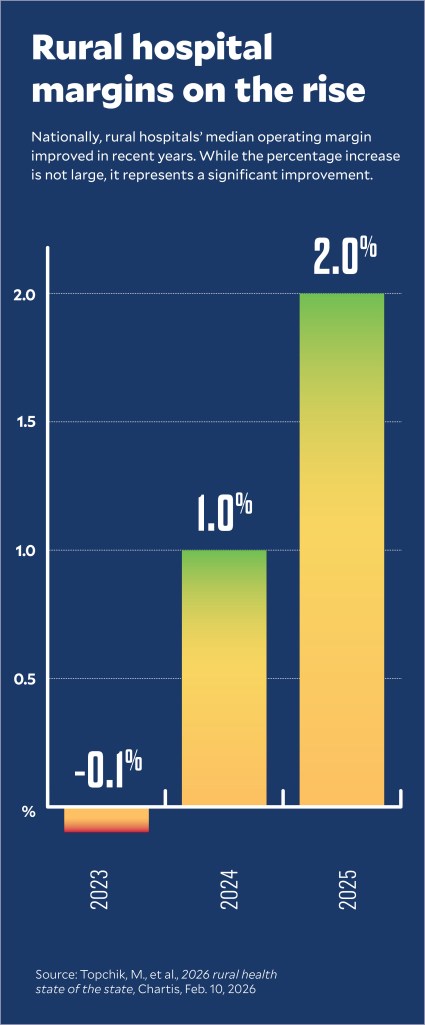
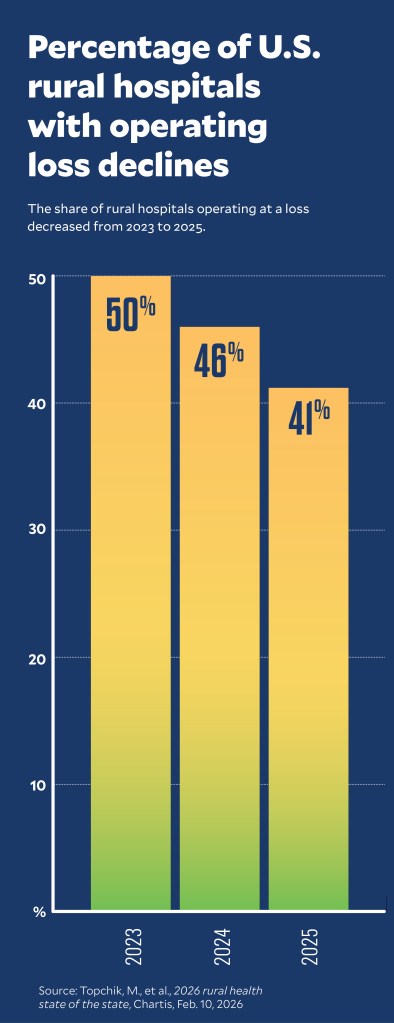
The finding of overall improvement in rural hospital finances nationwide came from Chartis in its annual report tracking their finances.a From 2023 to 2025, the report said, U.S. rural hospitals’ median operating margins improved, while the portion operating in the red steadily decreased.
“Those numbers did improve slightly, and a big part of that is the Medicaid expansion,” said Michael Topchik, partner and executive director of the Chartis Center for Rural Health.
In 2025 in Medicaid expansion states, Chartis found 34.9% of rural hospitals operated in the red, while 52.2% had negative operating margins in non-expansion states. Expansion-state rural hospitals also had a higher median operating margin at 2.9%, compared with -0.7% for those in non-expansion states.
Rural health initiatives lead the way
The improvement came amid a growing number and variety of initiatives aimed at bolstering the finances of rural hospitals. For example, rural hospitals in Pennsylvania recently concluded a model that sought to drive changes while improving their financial health.

Leaders participated in the model out of desperation, said Janice Walters, CHFP, MSHA, CEO of the Harrisburg, Pennsylvania-based Rural Health Redesign Center.
“It was the only way they could save their hospital,” she said. “But if we didn’t have people that are willing to go first and try something different, there is no innovation.”
One indication of the amount of work remaining was Chartis’ finding of little reduction from 2023 to 2025 in the number of rural hospitals in danger of closing.
The risk was demonstrated by the closure of 18 rural hospitals over the past three years, as tracked by the Cecil G. Sheps Center for Health Services Research.b However, there were 11 closures in Medicaid expansion states and seven in non-expansion states.
These statistics are emblematic of the variation that characterizes the nation’s rural healthcare market.
State variation in rural hospital financial performance
The picture becomes more complicated at the individual state level. Chartis found that rural hospitals in most states improved their finances from 2023 to 2025, but improvements varied widely, as did instances of deterioration.c
Among Medicaid expansion (Y) and non-expansion (N) states, those with greatest percentage-point decreases in share of rural hospitals with negative operating margin included:
- Kentucky 38 points (to 8.3%) Y
- Arizona 34 points (to 6.3%) Y
- Vermont 33 points (to 42%) Y
- Iowa 29 points (to 13%) Y
- New York 26 points (to 57%) Y
- South Carolina 25 points (to 27%) N
Similarly, states that saw the biggest percentage-point increases in their share of rural hospitals with negative operating margins included:
- Maryland 15 points (to 40%) Y
- Texas 14 points (to 46%) N
- Nebraska 7 points (to 49%) Y
- Oregon 6 points (to 50%) Y
- Hawaii 6 points (to 46%) Y
- Pennsylvania 5 points (to 45%) Y
State drivers of rural hospital performance variation
Topchik said a range of state-specific healthcare policies are likely driving that variation. For example, in New Mexico, where rural hospital negative operating margins decreased 14 points from 40% to 26%, the state created in 2023 the Rural Health Care Delivery Fund to cover operating losses and start-up costs for new or expanded services at hospitals and other providers.
Also running during the time frame examined by Chartis was the Pennsylvania Rural Health Model (PRHM).d From 2019 to 2024, the state-run model aimed to bolster rural hospitals’ finances through multi-payer global budgets.
Walters, who served as executive director of the PRHM, said it boosted rural hospitals’ financial outcomes mainly by reducing expenses and creating predictable budgets. An expected new iteration of the model is expected to further improve the hospitals’ finances while driving service redesign at those facilities. (See the sidebar at the end of this article.)
States may soon see a boom in such rural provider models because as many as 15 states plan some form of alternative payment model for their rural providers as part of their applications for newly available federal funds. CMS recently released the first round of $50 billion scheduled for distribution to the states through the Rural Health Transformation Fund.
Some rural hospitals also have benefited from Medicaid state-directed payments (SDPs), which can increase Medicaid payments to as high as average commercial rates. Expansion state hospitals especially benefited, given their higher shares of Medicaid enrollees, said Topchik.
For instance, SDPs improved Medicaid rates for Owensboro Health, which operates a 477-bed hospital in rural Kentucky, according to Fitch Ratings. That SDP revenue contributed to the rating agency last year upgrading the organization’s revenue bond rating.
Some states also have temporarily shored up rural hospital finances through grants or loans. The $300 million California Distressed Hospital Loan Program has provided interest-free loans to independent hospitals since 2023, with some having the balance forgiven by the state since then. New legislation would offer another $300 million and extend eligibility to hospitals that are part of health systems. Hospitals could qualify for forgiveness if adversely affected by the One Big Beautiful Bill Act.
Wider trend in healthcare financial improvements

Rural hospitals’ financial improvements also came amid broad hospital and health system financial improvements since the 2022-2023 time frame, according to Fitch Ratings.e In recent post-COVID-19 years, hospital volumes have surged, while organizations have focused on delivering productivity enhancements and process improvements. These have helped improve cash flows for investment and maintain balance sheet strength, according to Fitch.
Many rural hospitals have lagged in overall financial improvement because they lacked the ability to afford increasingly costly technology upgrades or to implement the value-based payment (VBP) push from Medicare and Medicaid, said Teresa Waters, PhD, dean of the School of Public Health at Augusta University in Georgia.
“That’s just a lot to ask of small organizations who are also facing other challenges,” Waters said.
Strategic options for rural hospitals
Some rural hospitals also have used strategic moves to improve their financial positions in recent years.
“There are a lot of options available to rural hospitals, and they are exploring them,” Waters said, also noting that “there are no magic bullets out there.”
Here are four of the most frequently pursued options.

1 Conversion to rural emergency hospital (REH). REH conversions are the newest and potentially the most fraught options for local hospital leaders because they provide higher payments but only in exchange for eliminating inpatient services. Since January 2023, 44 rural hospitals have converted to REH status.f The Chartis tracking data did not include REHs.
One hospital administrator and CFO said REH conversion not only turned around the finances of his hospital but also allowed it to add services, such as a walk-in clinic with weekend hours that his community sought.
“Rural communities need to embrace that concept — that they need to be what their community needs them to be and not try to be everything for everybody,” said Aaron Herbel, administrator and CFO of Mercy Hospital in Moundridge, Kansas.
2 Regional partnerships. Such partnerships among independent rural hospitals aim to pool resources to expand access to care, increase the use of health information technology and explore alternative healthcare delivery models. As of May 2023, about 40 such regional partnerships had been formed around the country comprising mostly independent hospitals.g
Topchik highlighted the emerging push toward rural hospital clinically integrated networks as another trend to watch.

One variation has been the emergence of independent rural hospitals sharing specialists’ services, said Steve Wasson, chief data and intelligence officer for Strata Decision Technology. Under these arrangements, one hospital may employ a specialist — an oncologist, cardiologist or orthopedist, for instance — who then provides services across rural hospitals within the same region.
“It’s saying, ‘Look, I can’t operate all these service lines effectively and profitably and serve my community the best way possible if I try to have everything for everybody,’” Wasson said.
3 Consolidation. Merging with a health system or other independent hospitals has benefited some rural hospitals. A majority (55%) of rural hospitals that closed from 2011 to 2021 were stand-alone hospitals, according to a 2024 analysis conducted by Dobson DaVanzo & Associates, a healthcare consulting firm.h The study also found that average total margins for acquired rural hospitals improved from 1.5% prior to affiliation to 2.3% post-affiliation.
Consolidation has provided some rural hospitals with the technological infrastructure and back-office functions to participate in VBP, Waters said.
Strata tracking data has found an ongoing financial divergence, with hospitals that are part of systems outperforming independent organizations, Wasson said.
Even though mergers and acquisitions slowed in 2025, at least 11 rural hospitals either joined health systems or partnered with another hospital that year to form a system.
Examples are:
- Hugh Chatham Health, an 81-bed acute care hospital in Elkin, North Carolina, which joined Atrium Health Wake Forest Baptist, part of the larger Advocate Health system
- Comanche County Memorial Hospital, a 265-bed rural hospital in Oklahoma, which announced an agreement to acquire Southwestern Medical Center, a 199-bed rural hospital, and form a health system called Memorial Health System of Southwest Oklahoma
4 Conversion to critical access hospital (CAH). Conversions to CAHs have increased in recent years and are used by some to garner higher payment rates in exchange for a low number of inpatient beds. Forty-five hospitals have converted to CAH status over the past three years, according to one tracker.i
Last year, Fitch specifically cited the CAH status — and the higher Medicare payments that come with it — in supporting Grande Ronde Hospital’s expectation that operating EBITDA margins would hit 9% by the end of fiscal 2026. That result would be a big turnaround from the rural Oregon hospital’s 1.9% operating EBITDA margin in fiscal 2025, which was driven by inflation, turnover and elevated expenses from a 2022 expansion project.
Future uncertainty
Rural hospitals face potentially significant financial challenges from looming federal policy changes. But financial trends in recent years show the potential for state initiatives and strategic moves by rural hospitals to determine the financial future of those organizations.
Footnotes
a. Topchik, M., et al., 2026 rural health state of the state, Chartis, Feb. 10, 2026.
b. The Cecil G. Sheps Center for Health Services Research, “195 rural hospital closures and conversions since January 2005,” page accessed March 11, 2026.
c. The Chartis Group, National and state data tables, accessible at info.chartis.com/ccrh-policy-institute-2024-state-data-0 and info.chartis.com/ccrh_state_data_2026.
d. Commonwealth of Pennsylvania, “Pennsylvania Rural Health Model,” page accessed March 12, 2026.
e. Fitch Ratings, U.S. not-for-profit hospitals and health systems outlook 2026, outlook report, Dec. 8, 2025.
f. The Cecil G. Sheps Center for Health Services Research, “44 hospitals are currently operating as rural emergency hospitals,” The University of North Carolina at Chapel Hill, page accessed March 11, 2026.
g. Hostetter, M., and Klein, S., “How regional partnerships bolster rural hospitals,” The Commonwealth Fund, May 15, 2023.
h. Dobson, A., et al. The potential for hospital system integration to improve the financial outlook of rural hospitals in the United States, white paper, Dobson DaVanzo & Associates, LLC, Nov. 22, 2024.
i. Flex Monitoring Team, “Critical access hospital locations list,” page accessed March 10, 2026.
Right-sizing, refocusing services are key to rural hospital survival
The future of rural hospitals will require changing how they are paid and what they do. Both will be a challenge.
A growing number of initiatives aim to transform the payment model for rural hospitals to mitigate the decades-long financial struggles of those organizations. But some suggest the new payment models’ long-term success will depend on rural hospitals responding to these initiatives by right-sizing and refocusing their services.
A Pennsylvania rural health initiative

That was a lesson learned by Janice Walters, CHFP, MSHA, CEO of the Rural Health Redesign Center based in Harrisburg, Pennsylvania. She was executive director of the state’s Pennsylvania Rural Health Model (PRHM), which provided rural hospitals with all-payer global budgets to improve their finances and enhance population health outcomes.
The model, which ran from 2019 through 2024, was launched by the CMS Innovation Center and the Pennsylvania Department of Health.
Initial analyses found the model improved the finances of the state’s rural hospitals, overall, but did not improve core quality metrics for their patients.a
A shortcoming of the model was that its global budgets would financially penalize hospitals for giving up high-revenue, low-demand services, such as orthopedic surgery, in favor of focusing on the core needs of their local population.
“For most of our hospitals, while it improved their bottom line, it didn’t get them to margin,” Walters said, “It reduced their loss significantly. But it still wasn’t enough to say, ‘OK, I need you to give up the orthopedics or partner.’ Should you do an orthopedics partnership for your region? Because they still would have taken a hit to the global budget.”
Improving those results will require a payer commitment to maintain the funding for rural hospitals, as well as a commitment by the hospitals to transform, Walters said.
Transformation would mean a refocus on the core — and often unmet — needs of rural populations, including primary care, mental healthcare, substance use disorder treatment and transportation services.
“When we talk about right-sizing rural hospitals, I have one hospital CEO who will say to me, ‘Just tell me what you want me to be, and I will do that really, really well,’ because they’re exhausted from trying to keep their facilities open,” Walters said.
A new attempt to transform rural health
Pennsylvania has proposed a new version of rural hospital value-based payment (VBP) as part of its application for a share of the $50 billion federal Rural Health Transformation Program. Fifteen states have proposed using that funding for various types of rural VBP models.
The new Pennsylvania VBP model also will include components on workforce and data-driven solutions, according to the application.
“The first program was a good test,” Walters said. “We figured out what works and what doesn’t work, and we take that and iterate and build a better, next generation program with fixed facility payments.”
Payment-driven transformation aims to allow rural hospitals to stop chasing commercial patient volumes for costly, high-margin services, like imaging and elective surgery.
“It’s about defining what the rural institution can do and what they can do really, really well and then let them be expert in it, versus them having to chase [volumes],” Walters said.
The problem is that the volume is not there, so the hospitals can’t deliver enough services to match their money, she said.
Transformation approaches also can include rural hospitals partnering with urban health systems for telehealth from specialists, instead of taking on their high costs of employing the needed specialists directly.
“Not all rural communities have the leadership skill sets necessary to pull some of this off,” Walters said. “How do we use technology to leverage and make sure the knowledge is there to do some of this? There will always be a need for rural communities to use broader health systems.”
Added services from these health systems could include expanded primary care, chronic disease management and testing for prevention and management. That allows the rural providers to narrow their focus. She said: “If you change the payment paradigm and say, ‘This is what we think you should be doing and this is what we’re going to make sure you’re held accountable for,’ then they can hopefully give up [trying to do all these services] and do primary care really, really well, do chronic disease management really, really well or do basic screens really, really well.”
Footnote
a. Dinesh, R.P., “Financial fix, quality flaw: lessons from Pennsylvania’s Rural Health Model,” Health Affairs, Feb. 11, 2026; and Chaterjee, P., et al., “Mixed evidence that rural hospitals’ finances improved with participation in The Pennsylvania Rural Health Model,” Health Affairs, July 20.