





Fast Finance
Hospitals see danger to SDPs in fraud fight
Changes targeting intergovernmental transfers were urged by a think tank aligned with the Trump administration.
Published
April 14, 2026
9:50 am
Hospitals are worried that a coming Trump administration fraud-fighting effort will go after Medicaid state-directed payments (SDPs).
The concern was raised by various hospital advocates responding to the administration’s solicitation for targets in its coming anti-fraud regulations, called the Comprehensive Regulations to Uncover Suspicious Healthcare (CRUSH).
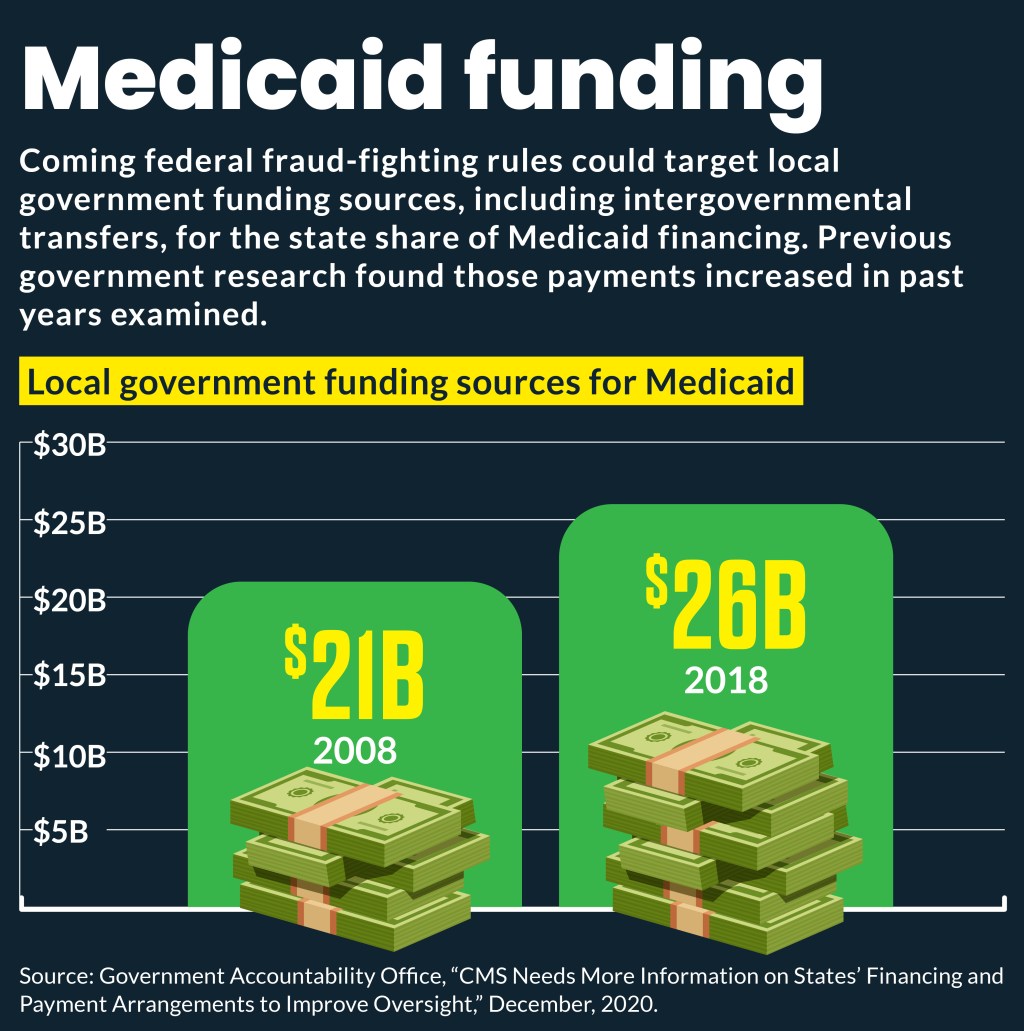
That request for information (RFI) specifically asked about fraud-fighting ideas in Medicaid related to “nonfederal share financing sources, including intergovernmental transfers (IGT).” IGTs are one of the ways states use to fund their share of Medicaid SDPs.
The RFI’s focus on Medicaid financing measures “signal that CMS is considering new federal restrictions” on how states finance their share of the program, according to a blog post by Dentons, a law firm. That would include the ways supplemental payments and SDPs are used to increase provider reimbursement.
“We are concerned that the RFI’s inclusion of questions about Medicaid supplemental payments and financing reflects a misunderstanding of how these long-standing Medicaid [payments] are used to advance program goals,” Jennifer DeCubellis, president and CEO of America’s Essential Hospitals, wrote to CMS.
The Healthcare Association of New York State (HANYS) stated that SDPs and Medicaid disproportionate share (DSH) payments are needed because Medicaid payments don’t cover the cost of services.
“HANYS urges CMS to consider the robust federal and state oversight already in place for these mechanisms and cautions against imposing additional administrative requirements, which would offer limited incremental value and risk diverting resources from care,” Marie Grause, RN, JD, president of HANYS, wrote to CMS.
Instead of new restrictions on SDPs, the Federation of American Hospitals (FAH) urged CMS to adopt various transparency measures around SDPs.
Why the concern
Hospitals’ concerns came amid concerns raised about IGTs and other approaches used to fund SDPs by the Paragon Health Institute, a center-right think tank closely aligned with the Trump administration. Congress included some Medicaid reforms advocated by Paragon in the One Big Beautiful Bill Act.
“As Paragon has documented, the federal share of total Medicaid spending has risen from about 60% to roughly three-quarters of the total bill, driven in large part by financing gimmicks like provider taxes and IGTs,” stated a recent Paragon blog post.
A 2023 Government Accountability Office report raised concerns about funding sources for SDPs. Specific concerns included:
- Weak fiscal guardrails
- No consideration of payment outcomes when renewing SDPs
- Gaps in transparency
The RFI also came amid recent CMS pushback on a $7.8 billion Florida SDP application that has resulted in an 11-month wait for approval. Similarly, California is still waiting on CMS approval of an $11 billion SDP submitted in March 2025 and funded by a one‑year hospital tax, according to a recent state budget document.
Other hospital worries
ACA marketplaces. FAH also warned off CMS on implementing additional ACA marketplace enrollee verification measures. Instead, it urged program integrity measures focused on agents, brokers and web brokers to target “the root cause of improper enrollments.”
The Trump administration has stepped up fraud enforcement in the ACA marketplaces. In 2025, a CMS review found an average of 1.6 million Americans each month were enrolled in both Medicaid/CHIP and a subsidized marketplace plan.
AI role. Hospitals also were leery of the use of artificial intelligence (AI), including machine learning and other advanced technologies, to assist in coding review, diagnosis abstraction, compliance oversight and hospital billing processes.
“While AI tools may be helpful as decision-support systems, they are not currently capable of fully replacing trained clinical coders, compliance professionals or clinicians,” wrote Kansas Hospital Association (KHA). “Overreliance on AI-generated outputs could introduce several risks that warrant careful consideration before incorporating such technologies into regulatory oversight.”
CMS’s most notable pursuit of AI-driven efforts to fight fraud, waste and abuse came in the recently launched Wasteful and Inappropriate Service Reduction (WISeR) Model. WISeR will test an AI-driven prior authorization (PA) process in fee-for-service Medicare for 15 procedures and services in six states over three years.
Hospitals had greater concerns with that model’s financial incentives for the technology companies conducting the PA over concerns about the technology it used.
Medicare issues
New MA plan authority. Hospital advocates also pushed back on the RFI’s proposal to allow Medicare Advantage (MA) and Part D plans to implement payment suspensions to providers suspected of fraud.
“Granting MA plans independent authority to identify providers for payment suspension or similar fraud-related actions would represent a significant shift in the existing framework,” said Charlene MacDonald, president and CEO of FAH, in comments submitted to CMS. “Expanding MA authority into areas traditionally reserved for federal fraud enforcement risks further blurring the line between government program integrity determinations and commercial claims management practices.”
Medicare claims. CMS also asked whether it should shorten the Medicare claim filing deadline from the current one-year standard to between 90 and 180 days. That aimed to address potential fraud vulnerabilities in certain high-risk service claims categories.
“Shortening the filing window would create significant administrative challenges and could produce unintended consequences for both providers and beneficiaries,” the Missouri Hospital Association stated in comments to CMS.
Dual enrollment. The RFI asked whether CMS should require providers to enroll in traditional Medicare as a condition of participating in MA networks and whether it should expand the preclusion list — a listing of barred providers.
The KHA urged CMS to carefully assess the operational implications of such policies.
“Many providers participate primarily in Medicare Advantage networks, and duplicative enrollment requirements could increase administrative complexity without clear benefits for program integrity,” KHA wrote to CMS. “In addition, expanding the preclusion list should ensure that only providers who pose clear program integrity risks are excluded from Medicare Advantage participation.”