





Fast Finance
States boost Medicaid budgets as enrollments decline
Some states are targeting hospitals for Medicaid rate cuts, amid tight budgets.
Published
April 20, 2026
9:38 am
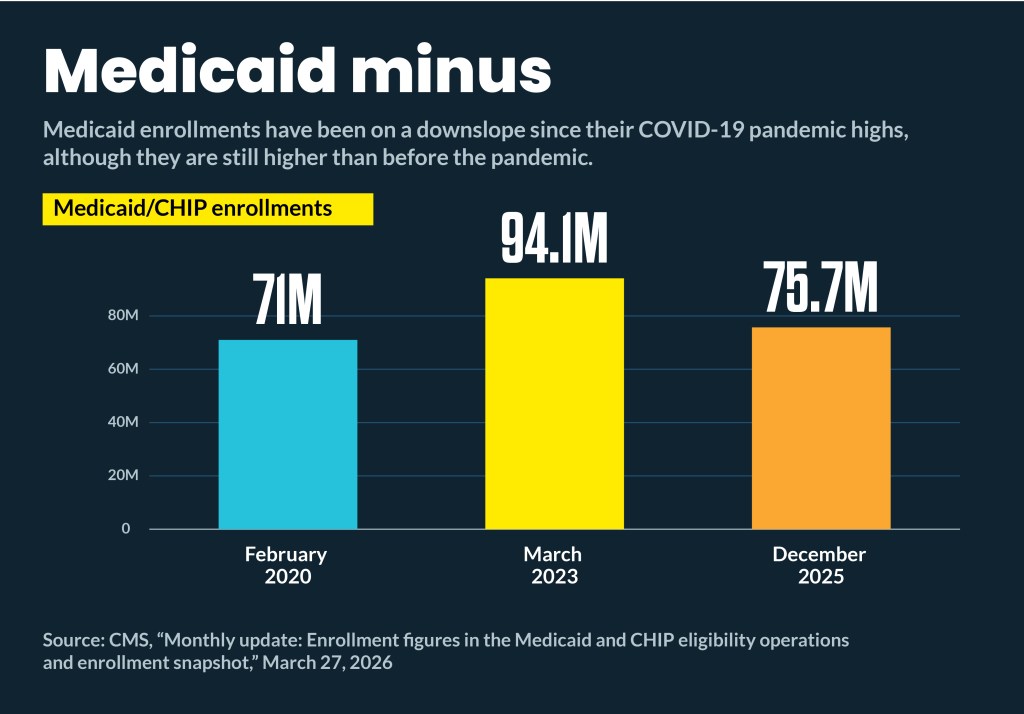
Amid ongoing and projected Medicaid enrollment decreases, most states are boosting their Medicaid budget proposals.
Nationally, Medicaid enrollment is shrinking. From December 2024 to December 2025, national Medicaid and CHIP enrollment has decreased 4%, from 78.9 million to 75.7 million, according to CMS. That has continued into 2026, with Wells Fargo analysts reporting a 2% decrease in the first quarter of 2026 in total Medicaid enrollment. Expansion enrollment is down about 1% quarter over quarter.
Meanwhile, Medicaid budget proposals from governors are seeking spending increases, including the following:
- $212 million, or 3.7% in Colorado
- $25.3 billion, or 13% in California
- $1.4 billion, or 4.7% Illinois
- $3.9 billion, or 11.4% in New York
At the same time, most of those states project that enrollments will decline:
- 3.37% decrease in enrollment by FY27 to FY28 in Colorado
- Decrease from 14.5 million to 14.3 million by FY26 to FY27 in California
- Decrease from 3.26 million to 3.1 million in Illinois
- 0.2% increase to nearly 7 million by FY27 in New York
Some states with biennial budgets already have enacted spending levels for the coming fiscal year. Those include Texas, which last year enacted a biennium budget to provide Medicaid $84.5 billion over FY26 to FY27. That was a $5.3 billion increase from the FY24 to FY25 biennial levels. The state projected that the 3.88 million enrollees in January 2026 would increase by 1.4% in FY26 and 1.4% in FY27.
Federal impacts
Some of the state projected enrollment decreases are from ongoing declines from COVID-19 pandemic highs, while others are from implementing the earliest provisions of the One Big Beautiful Bill Act (OBBBA). Those provisions included:
- October 2026, limits on Medicaid eligibility for certain immigrant classifications
- Dec. 31, 2026, start of work requirements for states not receiving a two-year extension
- Dec. 31, 2026, start of eligibility redeterminations every six months
The impact of those policy changes will vary widely by state: In Colorado, the Medicaid agency projected that 377,000 will drop off Medicaid when the work requirements and six-month eligibility checks begin.
Although OBBBA will reduce the rate of increase in federal Medicaid funds by $880 billion over the next 10 years, most major federal funding reductions don’t start until 2028.
OBBBA provisions also were cited as one of the factors driving Medicaid cost increases. For instance, the Illinois governor’s Medicaid budget proposal noted that it needed new FY27 funding to bring on an additional 450 staff to comply with the federal changes in enrollee eligibility and more frequent eligibility redeterminations.
North Carolina
The ongoing scramble to fund Medicaid spending increases includes a looming April 21 special legislative session in North Carolina. The governor asked for an additional $319 million, called a “rebase,” to cover a Medicaid funding gap.
After the state undertook an ACA eligibility expansion in December 2023, its Medicaid budget surged from $21.5 billion in FY23 to $36 billion in FY25. Adding more than 700,000 new enrollees brought total Medicaid rolls to 3.1 million residents by FY25. The state projects a 2026 to 2027 stabilization in the expansion population and a slight decrease in traditional Medicaid enrollment.
Republican legislators have balked at the rebase because it is just the first payment in an annual $819 million increase in Medicaid funding that the governor has projected. As in most states, the federal government covers most of North Carolina’s Medicaid costs, including $25 billion of the $36 billion cost in FY25.
“As state leaders negotiate the budget, the North Carolina Healthcare Association [NCHA] is emphasizing the importance of protecting access to care by prioritizing Medicaid funding and provider stability,” Stephanie Strickland, an NCHA spokesperson said in an email. “The Medicaid rebase must be fully funded to reflect the true cost of care.”
She warned that if the rebase is not fully funded, the administration should not resort to rate cuts to providers, particularly post-acute providers, where reductions could increase hospital lengths of stay and delay patient discharges.
“We support efforts to manage Medicaid costs, but not through policies that arbitrarily reduce hospital reimbursement,” she said. “A balanced approach is needed to protect patients, support providers and maintain a strong healthcare system across North Carolina.”
Colorado rates
Colorado hospital officials also have raised concerns that provider rates could be targeted to cover surging Medicaid costs.
On April 16, the Colorado Senate approved a 2% cut to Medicaid provider rates to save $95 million. The cut exempted maternal health and neonatal intensive care providers. The legislature still needs to reconcile differences between the Senate bill and a House-passed budget measure.
Medicaid provider rates have increased an average of 1.9% in the last five years, compared with the average annual hospital cost increases of 9%, according to the Colorado Hospital Association (CHA).
CHA co-authored a letter to legislators waring that rate cuts “will limit access to care for Medicaid members.”
“You are being asked to consider these cuts but not being given real and meaningful proposals to reduce bureaucracy related to Medicaid administration,” stated the letter.
New Jersy hospital funds
New Jersey hospitals also are bracing for cuts under the governor’s proposed budget. It would cut $89.5 million in state funding for acute care hospitals in FY27. The 6.5% cut would leave $1.29 billion for hospitals.
The biggest FY27 cut in hospital-specific appropriations is $103.7 million, or 53%. The state also would cut $496,000 from its three graduate medical education programs, which would leave $336.5 million.
The governor also proposed increasing the state’s charity care subsidy payments by $14.7 million in FY27, which would bring the appropriation to $83.9 million.
“For hospital finance leaders, this is about compressed margins, deferred capital, workforce pressure and harder decisions about which services remain viable in which communities,” Cathy Bennett, president and CEO of the New Jersey Hospital Association, said in emailed comments. “The math is unforgiving. When patients lose coverage, hospitals don’t stop treating them. We are calling on our elected leaders to hold the line on state funding. New Jersey cannot cut its way to a healthy population.”
A budget analysis from the legislature noted that federal law requires a gradual phase-down of both provider taxes and state-directed payments.
“In the case of hospital payments, implementing these reductions will require the state to make complex policy decisions that involve interactions among multiple categories of Medicaid payments. No final decisions have been made yet,” according to the analysis.
It also noted that one New Jersey hospital that closed last year also closed its stand-alone emergency department this year due to “financial distress.” The state is monitoring four other hospitals for “financial distress.”