





Healthcare Revenue Cycle Management
The Revenue Cycle of the Future: AI boom and workflow redesigns accelerate rev cycle transformation
Hospitals of all sizes are seizing a rare opportunity to improve the day-to-day business operations of healthcare.
Published
April 21, 2026
9:00 am
|
Updated
April 23, 2026
4:34 pm
With support from:
And:

“It’s ready,” you think as a notification flicks on the screen, relaying that your pizza has left the oven and is headed to a driver. Real-time updates such as this have become routine in fast-food delivery, giving customers instant visibility into a sequence that once required guesswork.
In healthcare, similar tracking technology could bring that same transparency to something far more consequential: prior authorization. That’s an approach Mayo Clinic in Rochester, Minnesota, is exploring now.
If Mayo Clinic’s pizza tracker-style solution works as planned, every stakeholder could soon see exactly where the prior authorization process stands as well as actions associated with the next step. Traditionally, this process has been fraught with multiple phone calls and emails among administrative staff, physicians and patients as they pull together clinical orders and documentation plus financial details, updates and communications related to scheduling.
The technology solution is one of many projects the organization is pursuing to modernize its revenue cycle.
“We’re advancing our use of predictive analytics, automation and AI to work more effectively and be less task-oriented from front-end to back,” said Nikki Harper, chair of revenue cycle — analytics, automation and diversified revenue for Mayo Clinic, an academic medical center with locations in Minnesota, Arizona, Florida and the upper Midwest. “We know we have to decrease cost to collect, and technology is a major play for how we can do that.”
This type of transformation isn’t just happening at large health systems. Across the country, hospitals of all sizes are accelerating revenue cycle technology adoption, driven largely by AI advancements.
Yet just slightly more than half of healthcare finance and revenue cycle leaders would describe their teams as “somewhat prepared” (44%) or “very prepared” (slightly more than 7%) for the revenue cycle of the future, according to a February 2026 HFMA survey. (See the exhibit below.) This puts intense demands on today’s workforce and leaders to level up skill sets, redesign workflows and refine governance processes in an AI-enabled revenue cycle world.
“It’s the most exciting time to be alive in revenue cycle,” said Candice Powers, chief revenue officer, USA Health, based on the Alabama Gulf Coast. “But my staff are also feeling that pressure, regardless of how much I try and shield them from it. Here in my own shop, we’re trying to bring everyone into a modern, more proactive mode. But staff are nervous. Staff can feel the tension. Staff can feel the urgency with which we’re being asked to act.”
Survey Question
Leaders fear their teams aren’t quite ready for the revenue cycle of the future
How prepared is your current revenue cycle workforce for the skills required over the next five years?
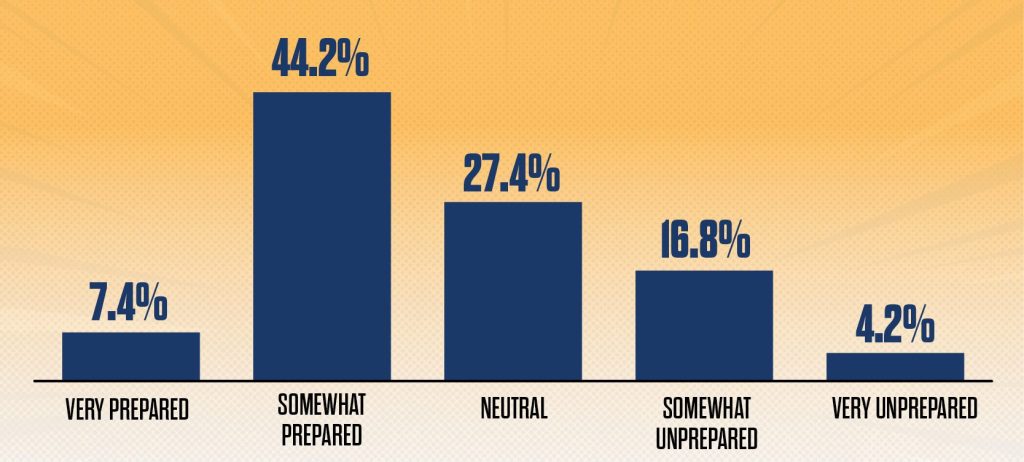
Source: HFMA Revenue Cycle of the Future survey, February 2026
A roadmap to transformation
Today, the U.S. revenue cycle management (RCM) market totals about $90.6 billion, according to industry estimates. By 2030, it is projected to reach nearly $308 billion.1
As the expense related to claim denials rises — and with hospital margins and patient loyalty at stake — the way AI is being applied to the revenue cycle is changing.2
The HFMA survey indicates AI pilots are moving to production-scale deployments across the revenue cycle. Among 95 healthcare finance professionals surveyed by HFMA, 27% say their organizations are actively deploying AI at scale across multiple functions, and 53% are conducting pilots in select areas.
McKinsey & Co. anticipates AI in the revenue cycle could lead to a 30% to 60% reduction in cost to collect, faster cash realization and a workforce refocused on patient value rather than administrative tasks. For patients, improved RCM could mean faster access to care and streamlined, less complex billing.3
In front-end operations, providers are exploring AI applications of self-healing data, where algorithms identify and correct missing or incorrect patient information in real time before submission, McKinsey found. Predictive analytics are flagging high-risk accounts during scheduling based on historical data. The patient financial experience is also changing with support from conversational AI and intelligent call deflecting.

Mid-cycle, leaders are focused on areas such as ambient documentation and autonomous medical coding, where AI analyzes clinical documentation and assigns codes, allowing claims to be processed within hours rather than days.
And many back-end advances targeting automation of appeals are well underway.
Michael Peterson, senior partner with McKinsey, noted that back-end functions — accounts receivable (A/R) follow-up, underpayment management, denials management and cash posting — are where many hospitals have made their first foray into AI. That’s because these tend to be labor-intensive, rules-governed tasks.
“Agentic AI can free staff up to focus on more strategic activities, spurring efficiency and productivity across the organization,” he said.

The technology boom, paired with accompanying workflow redesigns, is seen by many as a rare opportunity to improve day-to-day business operations of healthcare.
Colleen Hall, senior vice president of revenue cycle for Kodiak Solutions, hopes that healthcare leaders double down on change.
“When we’re out talking with the market and you ask how much time is spent fixing problems these days, it’s generally 75% or more of the time is spent on issues that are created somewhere upstream, and 25% is spent on being preventative,” she said. “And I think the revenue cycle of the future — so that we continue to thrive in the healthcare system that we have today — is going to have to shift those percentages and spend so much more time being preventative. And I think AI can help us with that.”
Survey Question
Change in revenue cycle skills and roles expected across functions
Over the next five years, where do you expect the most significant change in revenue cycle workforce roles and skills?
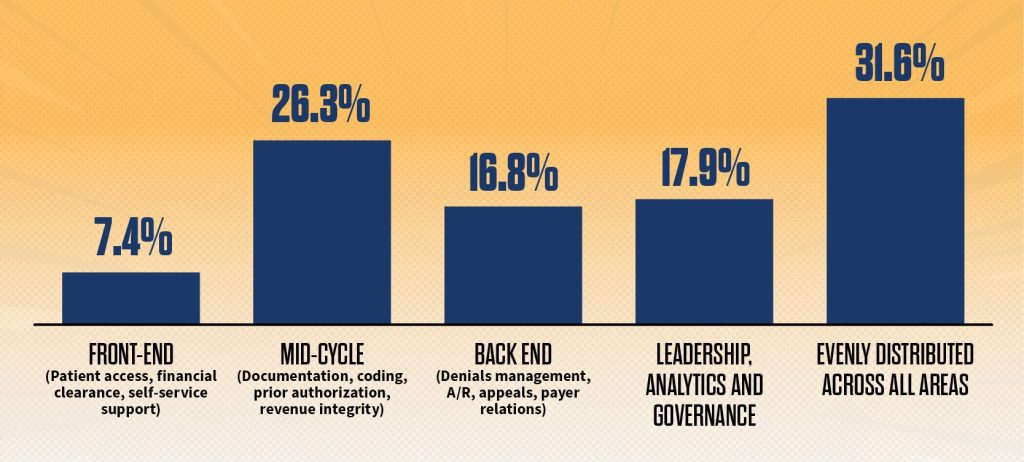
Source: HFMA Revenue Cycle of the Future survey, February 2026
Future revenue cycle workforce dynamics
The demands on today’s revenue cycle workforce to reach that future can be intense.
USA Health’s Powers gestured at a whiteboard wall that was scribbled from edge to edge with projects.

– Candice Powers, chief revenue officer, USA Health, based on the Alabama Gulf Coast
Hospitals are already operating with lean staff in a “new normal” of tight margins and rising costs, she said. While many hospitals stabilized with improved margins (about 1.3%–2%) in the past year, they face rising labor expenses, inflation and Medicaid cuts.4
“For decades, our industry has been trying to reduce the number of people and touches in revenue cycle,” Powers said. “A lot of health systems are skinny, almost anemic right now — and not just in manpower, but in skill set. Because the first area that tends to get cut is a department’s education budget. So, it’s a very precarious time.
“How providers survive in the short run here, the next one to two years, will determine where we’re at five years from now,” she said.
Near term, most revenue cycle leaders are focused on leveling up or reallocating staff given current workforce shortages and difficulty retaining experienced coders, documentation, billers and A/R recovery specialists. Some mentioned that they hope more strategic and creative work will ease burnout.
Industry leaders point to the following revenue cycle workforce trends in an era of tech-enabled transformation.
- Shifts toward higher level, specialized tasks. One area where AI is already having an impact on the workforce is coding and documentation, as ambient listening and autonomous coding take over mid-cycle processes. Many coders and documentation specialists are shifting to managing exceptions or reviewing workflows associated with more complex care.
Similar trends are expected across the rest of the revenue cycle. As repeatable, transactional task work is taken over by automation, leaders are hoping to redeploy, reskill or upskill workers into higher-value work, such as upstream problem-solving, exception-based strategy and patient experience.
Noted Mayo’s Harper: “People are understandably nervous about what automation and AI may mean for their jobs. But the focus should be ‘elevate, not eliminate.’”
She stressed that there still is a place for human talent in the revenue cycle of the future.
“Their place will still exist, but the skills used will change,” Harper said, giving the example of staff who currently are involved in claim status tasks that have some familiarity with payer behaviors. “Going forward, perhaps they move to the analytics side of things, so instead of working on individual tasks, they’re looking at such trends from a higher level. Or perhaps they are studying how to move metrics around the appeal type. Or perhaps they are going upstream to fix that reason for denial or delay, either with a claim edit or a physician clinician behavior. It will be an exception-based focus that they’re going to be moving to and using more critical thinking than they did before.”
Some areas of the revenue cycle will also be more likely to blend technology and human elements than others, particularly where the patient experience is at stake.

“In patient access and scheduling, agentic voice interactions will become much more common. But organizations will still need strong foundational templates, physician alignment and — most important — patients who are comfortable with those communications,” said Isaac Sieling, managing director, managed services, revenue cycle for Huron, an international consulting firm based in Chicago.
- Potential workforce gaps. Some reallocations of the workforce may have unintended consequences. One area of concern expressed by many is potential de-skilling as more routine work starts to disappear. In this scenario, organizations lose the bench strength of those who not only know every aspect of a process but also have been field tested and can therefore more easily spot exceptions or gaps or flex back to earlier modes of working during automation outages.
“It’s going to be so important that we still maintain that high level of workforce quality even when we start moving away from so many manual tasks,” Sieling said.
In addition, retraction in some areas of the RCM workforce may affect the longer-term workforce pipeline.
Gerard Brogan, MD, senior vice president and chief revenue officer at Northwell Health explained: “It’s getting harder to attract people into coding, because they look in the marketplace and see all these companies racing to create accurate, autonomous coding tools. It’s kind of like someone wanting to become a blacksmith for horseshoes when you see the Model-T coming out of the factories. Will you be able to find the workforce to do this work?”
Survey Question
Increased automation in the revenue cycle doesn’t come without discomfort
Which concern gives you the most pause about increased automation in the revenue cycle?
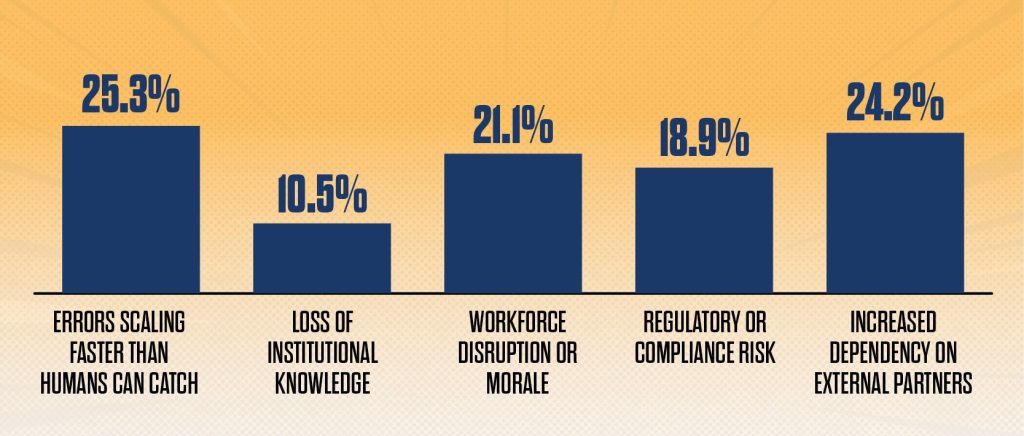
Source: HFMA Revenue Cycle of the Future survey, February 2026
Other trends to watch
Beyond technology and workforce shifts, leaders are keeping an eye on several broader dynamics that could shape the next phase of revenue cycle transformation.
- Greater interdepartmental collaboration. As focus increasingly moves away from transactional tasks toward strategic improvements in care delivery, it will be increasingly important for revenue cycle executives to share insights with clinical and technology counterparts on meeting payer requirements and workflow impact on payment processes. Whether they are working together on assessing technology platforms, processes to achieve incentives/avoid penalties around outcomes-based payment or the selection of formulary drugs, the best strategies tie operational and financial impact.

– Gerard Brogan, MD, senior vice president and chief revenue officer at Northwell Health
“Having the revenue cycle team strategizing with clinicians and with IT leaders is going to be critical to come up with care models that are of sufficient reimbursement to keep you afloat,” Brogan said.
- Uncertain payer relations. Payer relations are another major concern. Some industry experts noted that even having the best technologies and smart workflows can’t make up for shortcomings from a system where payer-provider incentives aren’t aligned.
“I would argue that the fundamental disconnect between payers and providers is not a technology challenge,” said Sieling with Huron. “We’ve had the technology needed to reduce friction within the system for years.”
He anticipates either better collaboration will occur or the industry is likely to continue to pursue the same denial-and-appeal cycle, only with different technologies.
“My hope is that we can find ways to the former,” he said.
- More complex vendor strategy. Vendor strategies will also evolve as consolidation among legacy RCM vendors occurs alongside rapid growth of AI startups. Kodiak’s Hall anticipates providers generally will use fewer and broader vendors to gain economies of scale and limit the amount of data sharing given their desire for cybersecurity.
“Health systems out there are looking to do more with fewer vendors. And when it comes to who they use, it’s also a risk play,” she said.
Among HFMA survey respondents, 37% describe their current vendor relationships as “functional but increasingly complex.” Almost one in five say they are “fragmented and difficult to manage.”
Most hospitals and health systems are expected to pursue a strategy that blends “buy, build or partner” based on specific project goals and constraints, making for greater complexity in strategy.
McKinsey’s Peterson said the right approach focuses on alignment with organizational priorities, whether that means retaining intellectual property by building in-house or achieving speed and scale through partnerships or enterprise platforms.
“Let the business objective inform the approach,” he said.
He also stressed the importance of a unified, enterprise plan that focuses on the longer-term whole versus individual pilots.
“You need a clear road map of what you’re trying to accomplish,” he said. “From there, it’s about tying everything together strategically — whether you’re building, partnering or buying — so each piece supports the broader vision. How you stitch all these things together in a holistic approach is really where the magic is unlocked.”
- Greater overlap of IT and revenue cycle tech management. Management structure may also look different, as several healthcare leaders noted.

“Revenue cycle is becoming less about finance and more about technology,” said Heather Dunn, senior vice president and chief revenue officer with Novant Health, a not-for-profit health system with a care network spanning North Carolina and South Carolina.
Given the prevalence of technology within the healthcare revenue cycle and its importance to an organization’s financial performance, Dunn envisions a scenario where revenue cycle technology could either be managed as its own entity within a health system, with executive oversight, or managed under the arm of IT.
An IT-orientation will also impact overall revenue cycle staffing, Dunn added.
“Revenue cycle teams will increasingly need staff who are driven by outcomes and know how to use technology and analytics to achieve them,” she said. “That’s where I see a shift. It used to be about diligence: coming into the office every day, knowing payer rules, knowing how to get a claim out the door. That is completely changing. It is now about knowing the technology to be built, and it’s about having the analytics to tell you where to drive that technology to hit the results that you’re looking for. That’s the shift that’s happening.”
Preparing the revenue cycle for what’s next
How can hospital revenue cycle leaders best lead their teams toward the revenue cycle of the future? Industry experts point to three lessons learned.
1. Don’t jump to tech first. “Instead of saying, ‘I want to use this type of automation or AI,’ start by questioning the problem you’re trying to solve,” said Nikki Harper, chair of revenue cycle—analytics, automation and diversified revenue for Mayo Clinic. “You never should put automation or AI on top of a broken process or people who need different training. Not only will you not solve the problem, but you’re often going to compound it with speed or scale and end up worse in the end.”
2. Be selective with pilots. Northwell Health has aggressively implemented AI and automation to modernize its revenue cycle management in coding, patient payments and ambient AI, among other areas. Gerard Brogan, MD, senior vice president and chief revenue officer at Northwell Health, credits the organization’s successes to working only with companies where the health system can see the technology already in operation and talk with users or else where they have a co-development structure with enough equity stake to justify the time and energy for staff given the team’s limited bandwidth.
“It’s very risky,” he said. “So, we would like to see that they have a couple of partnerships out there that are up and running, even if small.”
Users are especially important to assess the vendor’s willingness and speed to ingest feedback and turn around improvement, he said.
“We’ve had some very successful partnerships with those who are really willing to take the feedback and make changes, and then others who really just wanted to have us accept what they had put together, even though it really wasn’t solving our problem,” Brogan said.

– Sanjiv Baxi, MD, partner with McKinsey & Co.
3. Be brave. With margins tight, the room for error in technology investments is small. And while it’s wise not to be the first to adopt, there are costs to waiting too long. Assessment is needed around ongoing revenue leakage with legacy systems, operational inefficiencies, high manual labor costs, insufficient denials management to counter rising AI use of payers, inability to keep pace with payment reforms and reduced time for patient support.
“You can’t be paralyzed by the concern that technology is moving too fast,” said Sanjiv Baxi, MD, partner with McKinsey, noting that providers over the years will often say they are waiting for the technology to settle a bit or the right sort of vendors to come along.
The revenue cycle of the future won’t be kept waiting.
“Historically, providers could often afford to wait and see how things played out,” Baxi said. “But I think in this setting, waiting too long risks falling meaningfully behind.”
Footnotes
1. Grandview Research, “U.S. Revenue Cycle Management Market (2025-2030),” 2025.
2. Williams, J., “Battle of the bots intensifies over denials,” hfm, February-March 2026.
3. Peterson, M., and Baxi, S., “Agentic AI and the race to a touchless revenue cycle,” McKinsey & Co., Jan. 9, 2026.
d. Vizient|Kaufman Hall, New margin math, Trends report 2026, Jan. 22, 2026.
PHOTOS BY MARSHALL CLARKE; COVER ILLUSTRATION OF AN IMAGE BY MARSHALL CLARKE
This report was developed with generous support from its sponsors.
In a supplement to the report:
- James Hillenmeyer, Huron’s managing director, revenue cycle, defined shifts in the landscape.
- Sam Schwager, SuperDial’s co-founder & CEO, said a multimodal approach is key.
- Joe Kight, U.S. Bank Institutional Client Group’s Head of Healthcare, discussed ways finance leaders can drive impact.