





Fast Finance
Hospitals, insurers clash on 340B rebate costs
How regulators weigh the competing cost claims could determine whether CMS issues a new 340B rebate model.
Published
April 28, 2026
3:24 pm
Hospitals and insurers both urged federal regulators to ignore the cost projections of the other side in their comments on a coming redux of a 340B rebate model.
The comments came in response to a request for information (RFI) from the Health Resources and Services Administration (HRSA) seeking input on whether and how to implement a 340B rebate model. Rebates would mark a major change in the program, which has required drug manufacturers to provide up-front discounts on their products for most qualifying healthcare providers.
The effort to relaunch the program followed HRSA’s previously planned start of a rebate model on Jan. 1, which was withdrawn after hospitals won an initial stay on it from a federal court.
Hospital projections
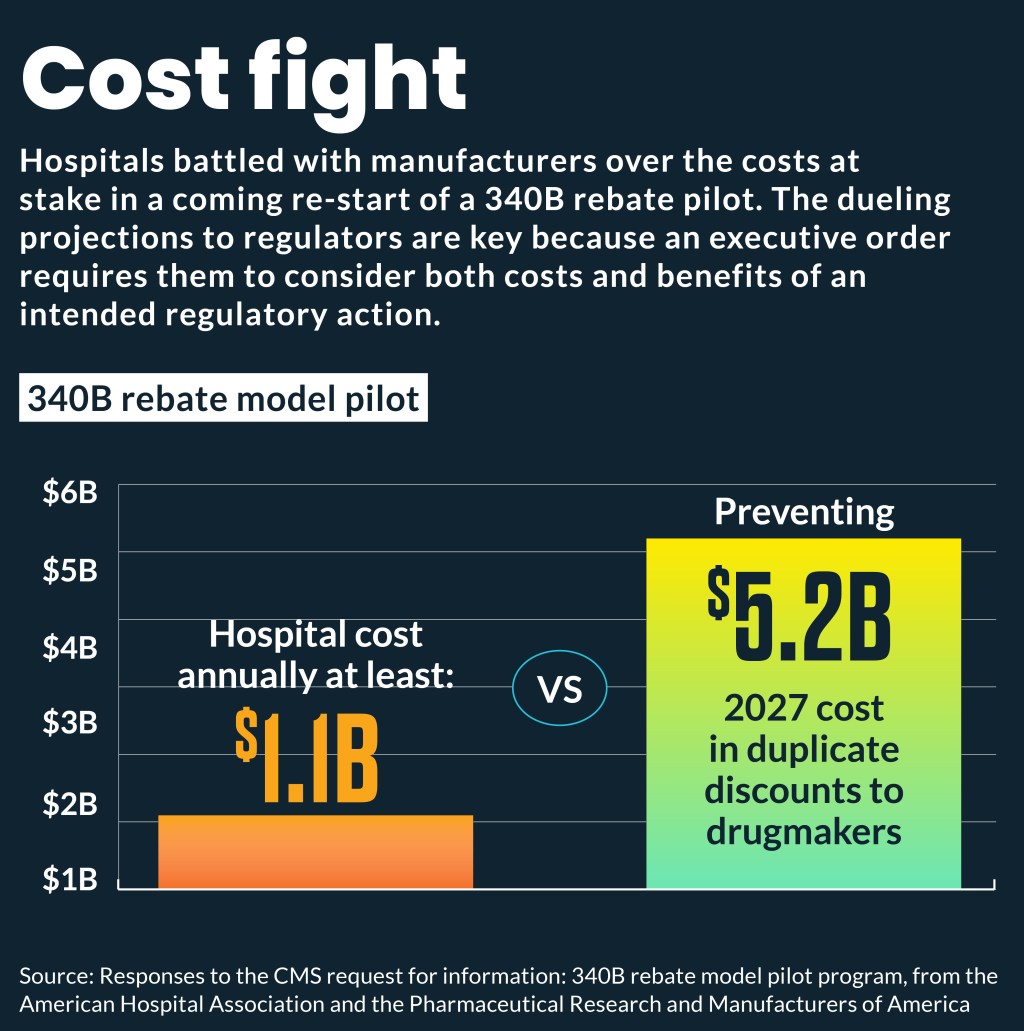
Hospitals and their advocacy groups raised a range of concerns about any rebate model, including a projection that it would add more than $1 billion in annual costs for those organizations — far outstripping any reduction in duplicate discounts.
“If it turns out that a rebate mechanism will impose billions of dollars of costs on covered entities while potentially saving far less for drug companies, there is no way a rebate program can survive scrutiny,” Chad Golder, general counsel and secretary for the American Hospital Association (AHA), wrote to HRSA.
The focus on costs compared to anticipated benefits is key, Golder wrote, because an April 2025 executive order required regulators “in deciding whether and how to regulate … agencies should assess both the costs and benefits of an intended regulatory action, as well as available regulatory alternatives, including the alternative of not regulating.”
“We are confident that once HRSA’s goals or anticipated benefits are clearly articulated, it will be clear that the rebate program involves too much guaranteed wasteful expenditure for too little potential gain.” Golder wrote.
Hospital executives, when told that HRSA projected $500 million cost for the revised model, “alternated between laughter to outrage,” Golder wrote.
AHA projected that merely hiring the one full-time pharmacist needed to oversee the rebate model at each of the 2,728 340B hospitals would cost $750 million, annually. Additionally, operational costs, such as vendor and third-party administrator fees, IT support and financial auditing costs, would conservatively cost $400 million annually.
Individual hospital cost
Conservative annual cost projections for individual hospitals to implement the rebate model, according to the AHA, would average:
- $150,000 in administrative costs
- $275,000 for one pharmacist
Some large 340B hospitals may need to hire as many as three pharmacists to oversee the model, which would increase the new annual labor cost for those organizations to $824,000, according to AHA.
Individual projections
Many hospitals and health systems also wrote to HRSA and projected how much implementation of the model would cost their organizations annually.
St. Tammany Health System, in Louisiana, projected that administrative and operational expense costs would range from $340,000 to $950,000.
St. Peter’s University Hospital, in New Brunswick, New Jersey stated that rebate billing and tracking software would cost it about $500,000.
Elliot Hospital, in Manchester, New Hampshire, estimated the model’s administrative impact at $1.5 million annually.
Float cost
Another cost of the rebate model is the amount of time that 340B hospitals would have to wait for payment on submitted claims. That so-called float was described by a federal judge who reviewed the initial rebate model as “an interest-free loan from the hospitals to the manufacturers.”
“Floating these sums imposes significant costs and burdens on 340B hospitals,” Golder wrote.
He cited the example of projections from Lexington Regional Health, a Nebraska critical access hospital, that the float would cost it from $150,000 to $300,000.
Manufacturer pushback
The Pharmaceutical Research and Manufacturers of America (PhRMA) wrote HRSA that a 340B rebate model would impose no more costs or burdens on covered entities than the replenishment models already used.
For example, PhRMA stated that the data providers would need to collect and submit in a rebate model are already captured in electronic health records; already required under 340B audit requirements; and currently submitted to manufacturers under the contract pharmacy policies of many drugmakers.
“We therefore urge HRSA to look with skepticism on unsupported or conclusory claims by covered entities that the requirements of a rebate model would cause them to incur substantial new costs or burdens,” wrote Elizabeth Carpenter and James Stansel, both executives for PhRMA.
They also wrote that even HRSA’s lower projected costs for providers were “inflated.”
Drugmaker costs
PhRMA instead underscored what it said were elevated current and future costs for manufacturers if a rebate model is not implemented. For example, the rebate model would create a reliable way to prevent duplicate discounts for the same drug in both 340B and from requirements of the Inflation Reduction Act (IRA). The IRA has mandated lower prices to Medicare for a growing list of drugs. The initial pilot was focused on those drugs.
PhRMA stated that such duplicate discounts will cost drugmakers an estimated $5.23 billion in 2027 alone.
Similarly, PhRMA stated that a rebate would prevent duplicate Medicaid discounts. Industry research estimated such dual Medicaid discounts totaled $1.5 billion in 2019, when the program was half its current size.
“A rebate model could equip manufacturers with the relevant information to identify these duplicate discounts in an efficient and targeted manner and resolve them consistent with applicable law,” the PhRMA executives wrote.
Challenging those costs
AHA pushed back on those claims by noting that drugmakers’ filings to the federal court that paused the initial rebate program claimed “chaos” would ensue at the start of this year if the rebate model was halted.
“But contrary to these assertions, there has not been ‘chaos’ over the past three-plus months,” the AHA wrote.
Manufacturers also projected $4 billion in 2026 losses from the resulting dual discounts. But those projections appeared to sharply decrease when drugmakers noted in a subsequent court filing that “potentially millions” in duplicate discounts and penalties were at stake.
“As ‘billions’ have become ‘millions,’ and as certainty has become ‘potentially,’ one thing remains clear: Manufacturers habitually overestimate the financial benefits (to them, of course) of a rebate mechanism for purposes of deduplication,” the AHA’s Golder wrote.