





Fast Finance
States overhaul certificate-of-need laws
Nearly half of the 35 states with CON laws have told the federal government they plan to loosen or eliminate them.
Published
May 5, 2026
11:10 am
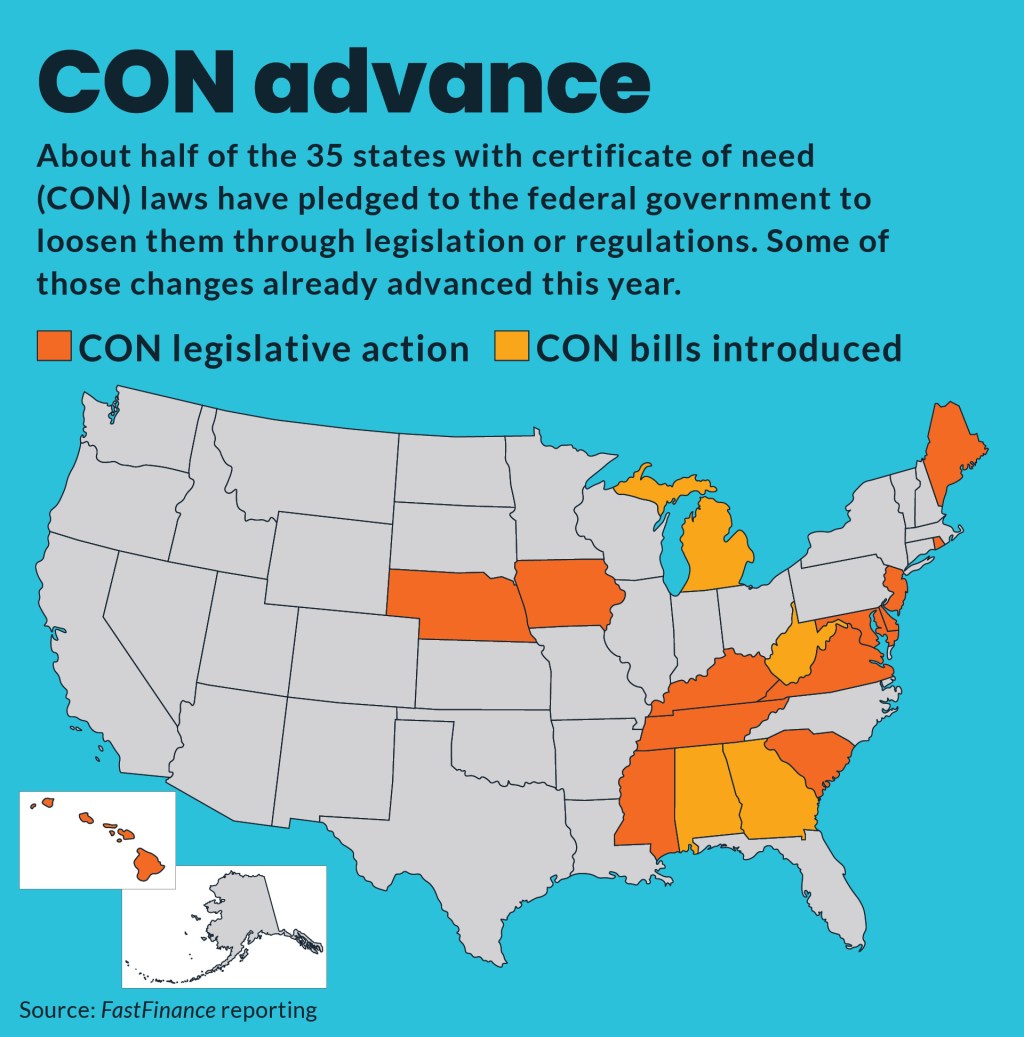
States have advanced a range of reforms to their certificate-of-need (CON) laws amid federal pressure to weaken or eliminate them.
The highest-profile change, so far this year, was Tennessee’s April 16 passage of a bill (SB1369) to repeal its CON requirements for acute care hospitals.
CON requirements for most acute care hospitals in the state will end in 2030. The law will replace the CON process with a hospital licensure process that will require them to treat Medicaid patients and provide charity care “comparable to similarly situated acute care hospitals,” according to the bill.
Hospital split
The legislative fight over the Tennessee CON repeal differed from those in many other states because hospitals were split over the bill, according to legislators. Hospitals traditionally support CON processes as needed to prevent over-supply of healthcare facilities that can undermine the finances of facilities treating low-income patients.
Lacey Blair, vice president of state government affairs for the Tennessee Hospital Association (THA), said at a March 18 Senate Health and Welfare Committee hearing that the THA was “neutral” on the legislation.
“I do feel that we will be actively involved as this process continues through the Health Facilities Commission, with licensure,” Blair said.
Sam Hazen, CEO of HCA Healthcare, headquartered in Nashville, has pushed for the repeal of CON laws.
“Certificate-of-need laws originally intended to control costs now do the opposite, limiting competition, constraining supply and increasing prices,” Hazen testified at an April 28 congressional hearing. “Revisiting these laws would encourage innovation and improve access, especially in underserved areas.”
State Sen. Joey Hensley (R), who represents a rural area, worries that ending the CON program would not help rural hospitals, like Maury Regional Medical Center, which is in his district.
“The rural county CON isn’t what prevents hospitals from coming to rural counties now and doing away with it isn’t going to make hospitals come to rural areas,” he said at the March hearing
State Sen. Bo Watson (R), the bill’s sponsor, noted that CON reforms were incentivized by the federal Rural Health Transformation Program (RHTP) grants under the One Big Beautiful Bill Act (OBBBA). OBBBA will provide $50 billion in rural grants through RHTP and the size of those grants is partly based on state policies, such as efforts to loosen CON laws.
“We cannot continue to do what we have been doing and expect healthcare to get less expensive and to get more accessible to the people we represent,” Watson said. “Time will prove that this was a transformational moment for the state.”
The legislation also will end the CON process for freestanding emergency departments and cardiac catheterization facilities by 2028.
Federal pressure
Tennessee is one of 17 states that pledged to undertake either legislative or regulatory reforms to their respective CON laws as part of their applications for a share of the $50 billion in grants through the RHTP.
CMS scored states on their CON laws and reform plans to determine how much RHTP money they will receive. States that committed to CON overhauls in their applications risk having grant money clawed back if they fail to follow through.
CON programs are operated by 35 states and Washington, D.C., according to the National Conference of State Legislatures. Many have undertaken changes to those programs in recent years, including South Carolina, which in 2023 repealed all CON requirements except those that relate to nursing homes and a select few related to hospitals.
Hawaii
Other CON bills that have advanced this year include a measure (SB2289) in Hawaii to exempt facilities from CON requirements if they provide certain health care services, serve federally designated, medically underserved rural areas or lower patient costs.
That bill was approved by the state’s Senate Health and Human Services Committee on Feb. 17.
John Lewin, MD, a senior healthcare advisor to Gov. Josh Green, MD (D), testified that the administration opposed the bill exempting ambulatory surgery centers (ASCs) from the CON process.
“Nonprofit hospitals in the state of Hawaii heavily rely on revenue from surgical procedures to offset losses they incur from providing crucial but nonprofitable services and providing millions of dollars in uncompensated care,” Lewin wrote to legislators. “Exempting surgical centers from certificate of need would allow for-profit providers to enter the market and divert significant revenue away from the hospitals.”
Paige Heckathorn Choy, vice president of government affairs for the Healthcare Association of Hawaii, said it was concerned it would exempt from the CON process hospice homes, pediatric and neonatal hospital care, as well as any facility in a medically underserved or rural area.
“Rather than improving access, such exemptions likely risk duplicative services, workforce dilution and erosion of quality in services, specifically for hospice patients,” she wrote to legislators.
Maine
A bill (LD1890) that became law in Maine on March 31 without the governor’s signature aimed to exempt most ASCs from CON review. It increased the capital expenditure threshold for facilities that would require CON approval from $3 million to $7.5 million and index further increases to the official inflation rate.
The Maine Senate also rejected on March 3 a separate bill (HP1471), which would have expanded the CON review process to sales of healthcare facilities involving private equity (PE) investors.
Jeffrey Austin, president of the Maine Hospital Association, testified that the legislation raised some concerns, including the addition of two new criteria to CON reviews.
Maryland
Maryland legislators also raised concerns from hospital advocates with legislation (HB944) to target PE investors in healthcare by requiring CON approval for mergers.
Andrew Nicholas, senior vice president for government affairs and policy for the Maryland Hospital Association (MHA), said the organization opposed the bill.
Although the hospital group shared the concerns of the bill’s advocates about increased PE healthcare investment, the language would exempt acute care hospitals but not health systems, of which many hospitals in the state are part.
“Given that the threshold for review in this bill is [that] either party having $10 million in assets, every transaction that a health system undertakes that is listed in this bill would be subject to this review, including fairly low risk transactions, like leasing office space,” he said at a hearing. “We think that creates a fairly significant burden without a lot of reward or something to be gained from it.”
Other action
Michigan. Introduced legislation (HB5709) March 11 to exempt from CON approval outpatient imaging services.
Kentucky. A committee approved a bill (HB407) on March 5 to modify the CON law, including allowing applicants to appeal adverse decisions to an appeals court.
Virginia. Defeated two bills (HB201 and SB168) that would have created CON exceptions for independent outpatient or ASC facilities and for maternal and perinatal health services.
Signed into law on April 13 a bill (HB1337) to provide expedited CON review of certain projects.
Delaware. On April 21, the Senate cleared a bill (HB17) for the governor’s signature that repeals required CON approval (called “certificate of public review”) for the acquisition of major medical equipment, although dollar limits apply.
Iowa. On March 5, the legislature cleared legislation (HF2635) that would increase the financial thresholds for capital expenditures and new equipment to subject provider facilities to the CON.
Nebraska. Signed into law a measure (LB437) to increase the amount of time — from one year to three years — that a new or modified CON approval is valid.
South Carolina. The House passed a bill (H4799) on March 26 to exempt veterans’ nursing homes from the CON process.
Mississippi. On Feb. 4, the House signed into law a measure (HB3) to study the feasibility of exempting small hospitals from CON approval for dialysis and geriatric psychiatry services.