





Fast Finance
Medicare Advantage turmoil continues
Several coming MA developments could help health systems.
Published
May 12, 2026
9:21 am
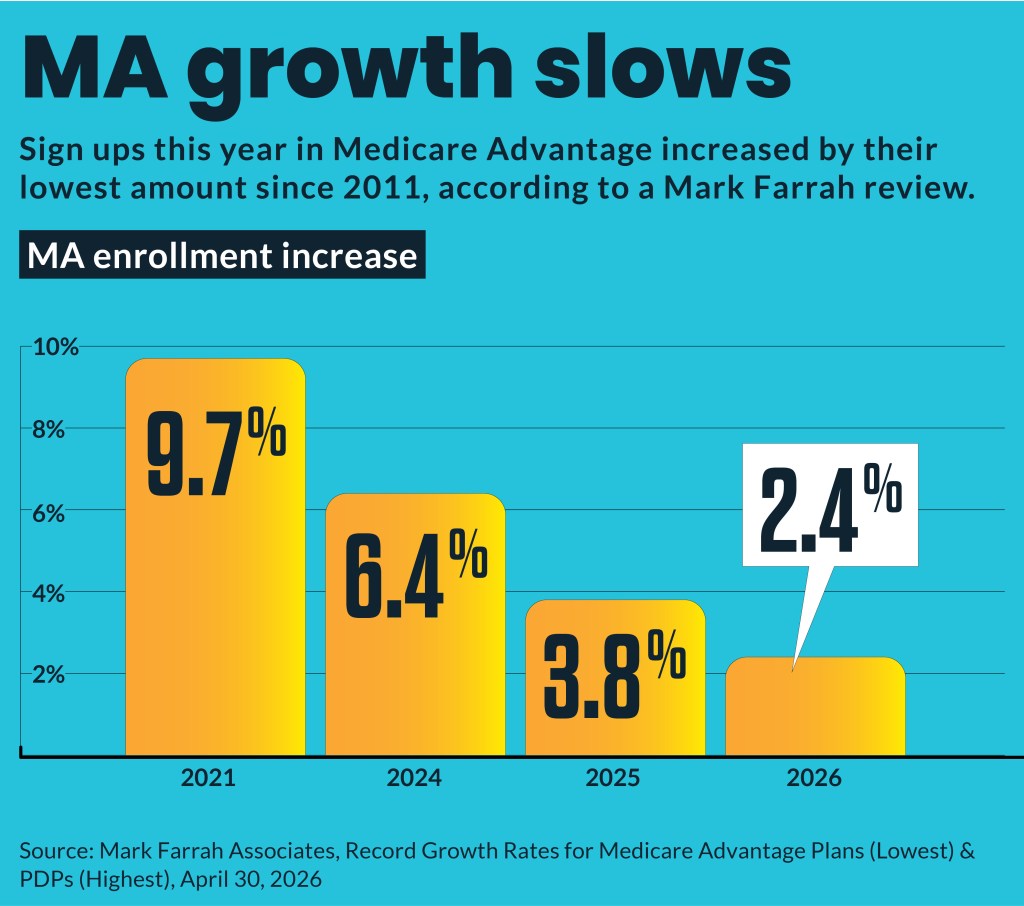
Medicare Advantage (MA) enrollment growth has slowed to its weakest in 15 years, but it remains the dominant Medicare segment.
MA enrollment, as of April 1, increased only 2.4% from April 2025, according to an analysis by Mark Farrah Associates. Enrollment increases have slowed from 3.8% in April 2025 and 6.4% in April 2024. The 2026 increase was the lowest membership gain since 2011.
However, MA remains the leading Medicare segment, with 51.8% of the 69.6 million people eligible for Medicare enrolled in an MA plan.
“We’re starting to see a slowdown and a stabilization of that growth because there is so much MA plan participation out there,” Shawn Stack, director of healthcare reimbursement consulting for Forvis Mazars, said in an interview.
Plan shakeup
A range of CMS rule changes led most insurers to pare back from underperforming markets and otherwise adjust their depth of involvement in MA, including:
- UnitedHealthcare left 109 counties across 16 states at the end of 2025, which affected about 180,000 enrollees.
- Six of the top 10 MA companies had year-over-year 2026 enrollment declines.
- The top 10 MA companies had an overall net enrollment gain of 1.5%.
- Elevance had the biggest enrollment drop, losing 15.8% of membership.
- Humana added the largest number of new enrollees, or 1.3 million.
- Forty-three states increased enrollment, led by Texas.
- Idaho, New Hampshire, Minnesota and Vermont had declines of more than 10,000 MA enrollees.
“These aren’t self-insured dollars, so they’re absolutely making a conscientious decision to leave what then I would call a potentially difficult market to be successful in,” Mike Ruiz, senior director, financial transformation advisory services at Premier, said in an interview.
Another payer trend is to shift more enrollees from PPO plans to HMO plans. The prior approvals required for specialist visits in HMO plans are another way MA plans will aim to control their plans’ costs amid worsening finances.
Providers walk
This year also has seen more hospitals and health systems terminating MA plans. At least 21 health systems are dropping MA plans for 2026, according to tracking by Becker’s Hospital Review.
“More and more we’re hearing from clients and different hospitals that if they can’t reach an agreement for an MA plan, they’re more apt to cancel the contract or get out of the contract because of issues in negotiations,” Stack said. “And I think a lot of that has come from the ability to accept patients out of network and still get that qualified payment amount that was readily made available under the No Surprise Act.”
The financial challenges facing MA plans also have led them to double down on administrative requirements, like prior authorization (PA).
CMS instituted new requirements for faster PA decisions. At the beginning of this year, payers must reduce decision timeframes (72 hours for urgent, seven days for nonurgent), according to CMS rules. That means payers increasingly will use AI to make those decisions.
“You’re just going to see denials shorten and, instead of taking four days, they’ll now take the 72 hours that they have, or sometimes even less,” Ruiz said. “I don’t see that being a great thing for systems, at least as of today.”
The same CMS rule also required use of the HL7 Fast Healthcare Interoperability Resources-based application programming interface to streamline PA and improve data exchange. However, that streamlining effort will work only if provider electronic health records, payer systems and operational teams are ready to use that new electronic PA infrastructure.
“My fear is that this has kind of gone under the line of vision for hospital leaders because it was pushed out as a CMS interoperability rule and prior authorization final rule for MA plans,” Stack said.
SNP growth
Special Needs Plans (SNPs) are the fastest growing segment of MA with nearly 869,000 enrollees added by April. Tracking SNP patients is increasingly important, especially for health systems that have invested in extensive population health management infrastructure.
SNPs are “a tiny, tiny footprint in the Medicare Advantage space, but absolutely something that I would be paying attention to in 2026 and certainly beyond, in terms of ‘Do I see those patients? If I do, am I doing what I need to do — from a utilization management perspective — to make sure I’m not getting things unnecessarily denied,’” Ruiz said.
For example, C-SNP plans are focused on chronic conditions, which requires providers to appropriately note, diagnose and code for those conditions. Failure to do so will result in up-front denials but also potentially extensive lost revenue among the range of follow-up care such patients require.
Ways forward
Instead of giving up on MA, Ruiz urges health systems to find good partners. CFOs should take a hard look at their portfolios with a deep data dive to find the plans in their markets with which they could build partnerships. That includes tracking their revenue from each compared with their expected revenue and whether the plans offer true value-based incentives.
Other factors to consider include:
- Focusing on at least four-star plans
- Targeting plans likely to last in the market long term
- Looking to well-established local or regional plans
‘No’ on downside risk
Health systems have found that in value-based arrangements in MA, they frequently do not perform well across the continuum of care when contracts include downside financial risk.
“What we’ve seen is a lot of these CFOs, understandably so, if they have them, they’re getting out of them,” Ruiz said about downside risk arrangements in MA. “And then, if they’re on the table, the short answer is ‘No.’”
MA plans lead all other types of insurance in the share of payments tied to downside risk, according to tracking data. However, MA plans stated that they have struggled to get hospitals and health systems to accept downside risk.
Downside risk arrangements require robust system capabilities for health systems, as well as a payer partner committed to providing timely data so that the provider can act fast enough to prevent losses.
“We’re recommending that they steer clear of [downside risk] until they can have that,” Ruiz said.
Stack said he is hearing more hospitals and health systems engaging in aggressive value-based payment arrangements with MA plans but it’s still “sparse” due to concerns over timely data.
However, expanded use of AI to provide rapid data turnaround with less administrative burden and cost could boost interest in such arrangements.
“That type of contract design is going to increase in the next couple of years just because of the enhancements that we’ve seen through advanced technology,” Stack said.