





Fast Finance
Amid ED surge, hospitals add diversion tools
One health system found better overall accuracy from its own home-based digital diversion tool than ChatGPT Health.
Published
June 8, 2026
11:55 am
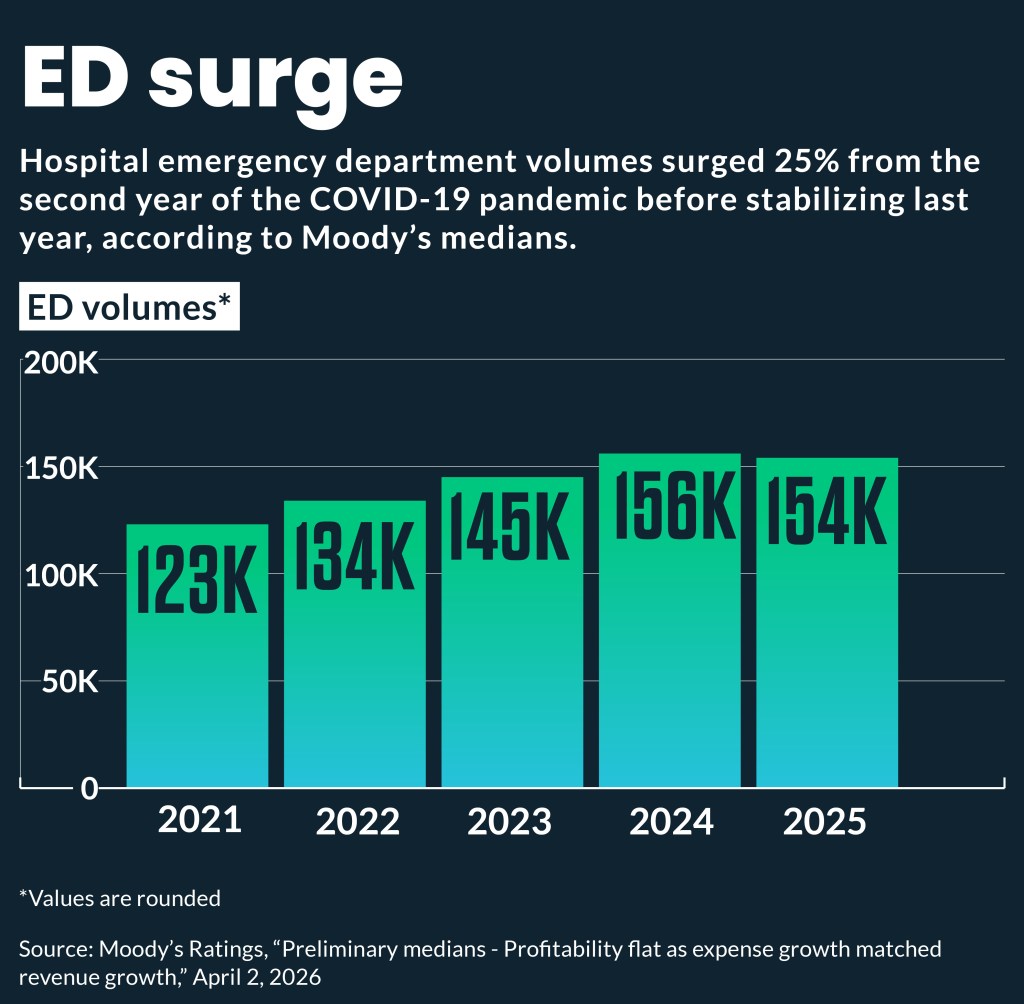
Surging emergency department (ED) volumes have led a growing number of health systems to launch digital tools to divert nonemergent patients to alternative sites of care.
Hospital ED volumes have increased 25% since 2021, according to the medians [subscription required] of rated hospitals tracked by Moody’s Investors Service.
High ED volumes have resulted in overcrowding and adverse patient outcomes, hospitals nationwide have reported. To mitigate those challenges, some health systems are deploying digital diversion tools.
“We have a real problem with overcrowding,” said Robbie Freeman, DNP, RN, PhD, chief digital transformation officer at Mount Sinai Health System. “So, the EDs are crowded and, if you don’t need to be there, we want to give you the option that’s most convenient to you, and so it helps us address overcrowding.”
Mount Sinai deployed a digital tool two years ago called Check Symptoms and Get Care, which is accessible as a button on both its website and app. The tool uses the Schmitt-Thompson Clinical Content telephone protocols — the same triage protocol used by its longstanding nurse triage call center — to assess patients’ symptoms and direct them to the best sites of care.
The tool then provides an option to click a button for an on-demand visit with the health system’s virtual urgent care, helps them schedule a primary care appointment or directs them to their nearest ED.
“The vast majority of those visits are virtual visits, so we know that’s a population of patients that historically would have walked into the ED or potentially urgent care who can now get that care on demand,” Freeman said.
The seven-hospital campus health system last year also expanded virtual services to those commonly sought in EDs by low-acuity patients, such as treatment for pink eye or diarrhea. Message Only Care, also available through Mount Sinai’s website or app, allows patients to type in their symptoms, answer clarifying questions and receive a treatment plan from a physician and prescription “within a few hours,” he said.
“Those are a couple of the ways that we can reduce the need for patients to come into the emergency department,” Freeman said.
Freeman was the former administrator for the health system’s largest ED, which cared for more than 100,000 patients annually. So, to him the need for diversion tools was clear.
“There’s a large percentage who don’t need to be in the hospital and don’t need to be in the ED,” he said.
Broader trend
The Mount Sinai digital diversion tools are among the earliest ventures into at-home diversion tools from health systems.
Cleveland Clinic is developing an AI-powered Digital Front Door that also plans to help patients find the right site of care before they leave home.
“With real-time data and a guided interface, this tool will shorten delays, lower congestion in emergency departments, and direct each person to the best care based on clinical need and location,” according to a description from the health system. The program is still in its early stages, said a spokesperson.
The emergence of provider digital screening tools follows long-standing offerings from health plans of a range of digital screening tools to help patients at home find the most appropriate sites of care for healthcare conditions.
ChatGPT competitor
The health systems’ home triage tools are already facing stiff competition from the growing use of consumer-facing GenAI options, such as ChatGPT Health, designed to guide users on where and when to seek medical care.
Mount Sinai studied the accuracy of ChatGPT Health compared to its digital triage tool and found its option provided more accurate recommendations to avoid both undertreatment and overtreatment.
“Because of the way we’re matching the symptoms to evidence-based guidelines that we’ve licensed from the Schmitt-Thompson protocol, our accuracy is much higher,” Freeman said.
Lessons learned
Several approaches were credited by Freeman with helping the health system to design an effective digital diversion tool.
First, was the use of a co-design process, which included patients and physicians in rapid-cycle design.
Secondly, they opted to incrementally add to the Check Symptoms and Get Care tool, with an initial focus on common urgent care-type symptoms for which patients may instead seek care in the ED. The system now is adding to the tool to address specialty care and more advanced options.
The health system also has closely tracked various components of its ROI.
“It may not be financially beneficial [to the health system] to have the patient in a lower-cost setting, and the ED is a higher-cost, higher-billing setting; when you switch that to a virtual visit or an e-visit, you’re not billing more,” he said. “But you’re doing what’s right for the consumer.”
Part of the ROI tracking is how many new patients come to the health system through the tool and the types of downstream care they obtain from the health system.
“We track all those downstream, so we can make the business case for how we’ve been able to grow the business,” Freeman added.