





Hospital and health system leaders need to consider factors besides age when replacing what could amount to thousands of assets in their organizations each year.
Just a decade ago, many healthcare organizations were eager to add the latest robotic surgery systems, linear accelerators, and other sophisticated equipment to keep pace with the competition—and keep physicians happy. But as margins have shrunk and access to capital has become more restricted, many providers recognize that replacing their equipment requires a more thoughtful, holistic approach, particularly as ubiquitous assets such as beds and lights require updates while more-strategic projects such as new construction command the C-suite’s attention.
Given these competing demands for capital, a strategy for proactive replacement planning is needed in which financial and clinical leaders come together to make more informed decisions for the organization. By leveraging existing data, replacement planning can help an organization achieve the following objectives:
- Reduce costs associated with parts, maintenance, equipment, and training
- Improve quality and reduce “near-miss” events associated with old or faulty equipment
- Enable leaders to reallocate underutilized assets
- Promote greater staffing flexibility across different sites
- Improve standardization across the enterprise, thereby further reducing costs
For many organizations, a comprehensive replacement planning approach would be a marked departure from the commonly used short-term, reactive strategy of purchasing new equipment when it breaks or when a department head says a purchase is mission-critical. Until recently, many finance leaders have been unprepared to discuss the ramifications of various equipment replacement choices with clinicians and physicians, who may escalate the conversation without presenting much evidence (e.g., “Patients are going to die if we don’t get this machine”).
Armed with better outcomes and cost data, leadership teams can have more meaningful conversations with clinicians that are based on fact, not hyperbole. Together, those two groups can discuss not only cost but also harm events and other quality and safety issues associated with healthcare equipment so they can make better choices together.
Utilizing a More Data-Driven Approach
Although the age of an asset is important, other considerations are crucial in a holistic replacement-planning approach, including the following.
Health of the equipment. Practical metrics for measuring the health and reliability of equipment include the number and frequency of work orders and the availability and supportability of parts.
Risk. Healthcare equipment can pose myriad threats to patients. The U.S. Food and Drug Administration (FDA) reports that infusion pumps, for example, may be plagued by software problems, battery failures, and other dangers. a Even hospital beds can pose a risk to patients. b
To understand the risks passociated with their equipment, leaders can check the FDA databases for medical device recalls, manufacturer and user facility device experience (MAUDE) events, and patient deaths related to equipment.
A growing risk is technology obsolescence, as outdated technology often poses a cybersecurity risk that can bring a service line to a halt. ECRI Institute has named ransomware and other cybersecurity threats as the No. 1 healthcare technology hazard in 2018. c
Workforce injuries are another risk. When patient lifts are not maintained properly or need to be replaced, for example, staff may suffer injuries, and workers’ compensation cases may rise.
In general, quality and safety issues typically supersede all other factors, making replacement of risky equipment a high priority for an organization.
Utilization. Changing volumes, based on unit-of-service trends, can help leaders gauge an asset’s utilization and determine whether they should replace or perhaps reallocate equipment to where it would have the greatest impact.
One service line at a North Carolina health system needed to replace its ultrasound equipment, which was significantly past its asset life, creating rising corrective maintenance costs—and frustrating staff. Meanwhile, another service line was looking to replace its relatively new ultrasound equipment with more sophisticated machines that offered a new testing option. Leaders reshuffled the newer equipment to the first service line and invested in better equipment where it mattered most. By embracing a “fleet” mentality, the organization was able to provide better care for its patient population, improve employee satisfaction, and fully maximize its investments.
Costs. The total cost of ownership for a piece of equipment has three components: acquisition costs, ongoing operational costs, and maintenance costs.
Acquisition costs include the cost to purchase the asset and other one-time costs, such as installation and any special diagnostic equipment needed to support maintenance. This figure also includes the cost of training for clinical engineers as well as clinicians and physicians.
Operational costs are related to day-to-day use and include supplies such as filters, bulbs, lead wires, flow sensors, batteries, and calibration gases. In many hospitals, supply costs often are overlooked in the planning process. At one hospital, leaders failed to anticipate the high cost of scopes for their robotic surgical system. Despite trying to offset these costs for a year, the hospital’s operating budget still took a hit.
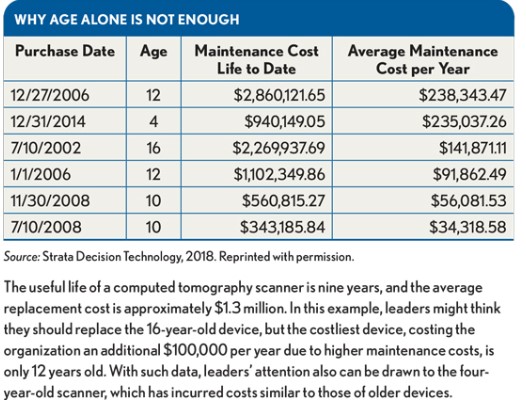
Maintenance costs include all the labor and parts required for preventive maintenance and for corrective maintenance in break/fix situations. Maintenance costs often are overlooked. Typically, when an asset is first installed, there is a high number of work orders (and thus, higher costs) as clinicians and staff become familiar with the equipment. Work orders drop off significantly until the equipment nears the end of its usefulness, when maintenance costs and downtime begin to increase. The exhibit below provides an example of the benefits that can be gained by reviewing maintenance costs. By reviewing such costs, leaders can understand their total cost of ownership and better prioritize which equipment should be replaced.
Prioritizing Equipment Purchases
All organizations are challenged to prioritize their capital needs within the constraints of available cash, including not only strategic investments to expand services but also investments to replace equipment and maintain the status quo. A multihospital organization may have 25,000 to 90,000 individual pieces of equipment in its inventory, whereas a single entity might maintain roughly 5,000 items. Assets that need to be replaced include not only advanced surgical and imaging systems but also the workhorses of patient care, which include supplies and equipment such as surgical lights, ultrasound machines, wheelchairs, and patient beds.
Unfortunately, many finance leaders do not have sufficient visibility into their equipment inventory to understand what they have and what needs to be replaced. By implementing effective processes and tools that provide such visibility, however, leaders can gain a better understanding of their entire asset database and the key metrics they should consider to make informed decisions. The objective should be to create a computerized maintenance management system that can provide insights that help leaders prioritize what to replace and when.
A common obstacle for an organization after a consolidation is having different systems in place at different facilities, yet even in such circumstances, it is possible today to consolidate the data from the different systems to provide leaders with a single system for better understanding what their replacement budget should be across the enterprise.
When setting priorities for replacing assets, leaders should ask the following questions for each asset:
- Has the number of corrective maintenance work orders increased year over year?
- Has the manufacturer sent an end-of-life notice on parts availability?
- Is the equipment associated with any security or quality risks?
- How many duplicate assets are available if this equipment is not replaced?
- How do maintenance costs for the past 12 to 24 months compare with the cash required to purchase a new asset?
Strategic and competitive considerations also should be reviewed when determining which assets to replace. Another consideration is the opportunity to reduce variation through standardization, which not only creates cost savings but also improves staff flexibility.
Leaders at a health system in Wisconsin wanted to flex some of their clinical staff across multiple hospitals in rural locations and in large metropolitan areas. But because the health system had grown by acquisition, equipment was varied across the enterprise. Using equipment data from across the system, leaders developed a replacement plan to standardize assets in key service lines and repurpose equipment to other facilities that were not part of the initiative. They negotiated lower pricing on equipment through their multiyear, group purchasing strategy, thereby reducing the health system’s acquisition costs and parts and supplies costs. And through flex staffing they also were able to reduce labor costs. These savings helped the health system shorten the timeline and reduce the overall purchase price for the standardization.
Negotiating with Vendors
By using a replacement planning approach, leaders may be able to exert more purchasing power with manufacturers. Typically, organizations have more leeway to negotiate the acquisition costs of equipment with vendors that also provide the supplies, parts, or service. These vendors can justify a lower acquisition cost if they can anticipate ongoing revenue over the life of the item. That said, leaders should be on the lookout for hidden operational costs over the long term.
For more effective vendor negotiations as part of a holistic replacement planning approach, leaders should consider the following strategic steps.
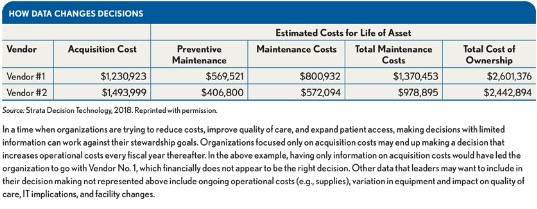
Educate clinicians and physicians on costs. Acquisition cost is just one component of the cost of an item to the organizations. The total cost of ownership—not just the acquisition cost—should be used to compare costs from at least two different vendors, as shown in the exhibit below.
Consider how switching equipment could lead to harm events. Changing equipment can create incompatibilities, such as rooms that are not designed for the proper use of new equipment. Having variation in equipment across the enterprise also can cause staff confusion. Even surgical beds can vary in operation, with staff mistaking a button to adjust the bed for a button to collapse it. For these reasons, leaders should carefully review any internal quality and safety events that have occurred, as well as risks reported by groups like the FDA, when reviewing vendors.
Use a group purchasing mentality. Instead of waiting until an asset breaks, leaders should establish contracts for multiple assets over several years to get the best price and promote a better partnership. Knowing the total inventory for each vendor can help leaders negotiate across the portfolio of products. If applicable, supply and maintenance costs should be included in these negotiations.
Lessons Learned
Healthcare organizations should adopt the following approaches for more holistic replacement planning.
Form a multidisciplinary replacement-planning team beyond the capital committee. Determining who owns the replacement planning process in an organization can be tricky, but leaders in clinical engineering, supply chain, operations, and finance all need to be involved in the decision making. Such inclusion could upset some within the organization—for example, entity or regional leaders who may not like sharing control with others across the health system, or service-line leaders who are used to getting their equipment replaced. The goals of this committee should be to use data to enhance consistency in determining when assets are replaced and improve accountability among operational leaders for all capital investment decisions (strategic and replacement). Convening a team that meets quarterly can ensure that replacement planning needs are prioritized appropriately in the capital process.
Make the data transparent. Some organizations maintain spreadsheets to determine which assets need to be replaced—a practice that can be as time consuming as it is error-prone. This manual process also fails to capitalize on the accurate historical data that are available in organizations.
Using an analytics tool for replacement planning with visibility into an enterprisewide maintenance management system can allow leaders across the organization to see what needs to be replaced, when it needs to be replaced, where it needs to be replaced, and what its estimated replacement cost is. Such a tool should incorporate data from multiple sources, including work order maintenance systems used by clinical engineering, IT, and facilities; plant ledgers that include equipment lease information; purchasing/contract systems that include maintenance contract details; department or service-line reports that include equipment utilization volumes; and data on end-of-life notifications and harm events. At a high level of sophistication, such an analytical tool can enable leaders to consider multiple data elements and weighting as they prioritize which equipment to replace. At a minimum, the tool should be able to capture the asset’s tag number, in-service date or date of purchase, taxonomy or asset group, make/model/description, and department or entity.
Start small. Not every organization needs to consider multiple data elements as they begin to approach equipment replacement holistically. Using just one additional data element beyond an asset’s accounting life can be helpful to prioritize which equipment should be replaced. In the first year of implementing equipment replacement analytics, leaders should assess which data elements can be used. Some easier data elements to review include remaining years of useful life (which compares the current age of the equipment with its expected life), asset performance (which reflects how frequently the asset breaks down, as recorded in the work order maintenance system), and supportability and parts availability (which is recorded in most computerized maintenance management systems).
As leaders gain more experience using data to drive replacement decisions, they can add other data elements to their prioritization process. Such elements include IT assessments that reflect potential security risks; data on employee and patient harm events that indicate potential quality risks; and volume trends across the department, service line, or facility.
Explore whether part of the equipment, rather than the entire item, can be replaced to extend its useful life. This approach also applies to operating systems that could be updated to prevent the expense of replacing a machine. A healthcare organization in Missouri that took advantage of an available vendor upgrade at one-quarter of the cost of buying new equipment for its lab not only extended the life of the equipment but also delivered better images and increased throughput.
Consider how replacement affects access to care. For some rural organizations that cannot afford to keep parts on hand, equipment failures prevent patients from accessing services they need. Leaders need to have a contingency plan in place to maintain effective patient care during any downtime, such as partnering with another organization to provide backup.
Consider removing an item from service. If volumes are not justified or an item’s break/fix costs are too high, leaders may decide not to replace a piece of equipment. Such decisions should be based on factors that go beyond costs, including patient access to care.
Planning for the Future
When discussing where to allocate capital, leaders often are drawn to more strategic investments, such as new medical buildings, rather than to replacing assets. Yet the dollars a hospital or health system requires to replace aging or faulty equipment grow year after year. Dipping into a contingency fund when equipment breaks is not an effective long-term strategy. By embracing proactive replacement planning, leaders can more confidently make decisions that positively affect the bottom line as well as the health of patients.
Footnotes
a. U.S. Food & Drug Administration, “Examples of Reported Infusion Pump Problems,” updated Dec. 13, 2017.
b. U.S. Food & Drug Administration, “Hospital Beds,” updated March 26, 2018.
c. ECRI Institute, “ Top 10 Health Technology Hazards for 2018: A Report from Health Devices,” Executive Brief, 2017.