





Cost of Care
Repurposing TDABC: Case Examples from a New York Hospital
Published
September 4, 2018
1:12 pm
|
Updated
December 16, 2022
1:28 pm
Adopting the principles of time-driven activity-based costing (TDABC) in measuring productivity and capacity utilization can help a healthcare organization identify the potential for performance improvements, such as opportunities to streamline staffing.
TDABC systems have been used sporadically across many large-scale industries as a management tool to measure costs, but they have not gained universal appeal in the healthcare industry. Resource constraints in the face of an unpredictable payment environment and the pressing need to implement electronic health record systems have created an impediment for healthcare organizations to embrace the model. Moreover, a widespread perception that TDABC is too technical and esoteric conceptually, and that it therefore requires highly specialized knowledge and skills to implement, has created a further barrier to its use.
The experiences of Lincoln Medical Center, a community-based healthcare facility in New York, provide compelling evidence of the practical utility of repurposed TDABC and the potential benefits that can accrue to healthcare organizations undeterred by such obstacles.
TDABC Demystified and Repurposed
Lincoln Medical Center moved forward with its adoption of TDABC principles based on the premise that this methodology has been adopted successfully and used frequently in other industries as a reliable tool to measure cost in a department. The organization’s leaders recognized that utilization of the ABC methodology has led to the achievement of higher levels of efficiency and cost reductions. By demystifying TDABC and establishing its effectiveness in capturing the complexities of various components of operations, Lincoln Medical Center has fostered its acceptance as a reliable and valid strategic planning tool among clinical, operational, and business managers.
Located in Southern Bronx of New York City, Lincoln Medical Center is an integral part of the NYC Health and Hospitals system, the largest municipal healthcare system in the country. Lincoln is a full-service acute care hospital, with a nationally recognized Level I trauma center. The following two case examples exemplify how Lincoln Medical Center has repurposed the TDABC approach to achieve substantial benefits.
Case Example No. 1: The Central Sterile Department
In the summer of 2017, Lincoln’s CEO and chief nursing executive (CNE) directed that an operational review of the central sterile department’s productivity be performed to ascertain whether the department’s annual utilization of 29 FTE technicians was justified. To support this effort, a staffing model was developed using the principles of TDABC to analyze the department’s overall capacity utilization and the productivity of each functional area.
Constructing the staffing model included the following three fundamental steps.
Identify functional areas. In the TDABC model, all major activities performed in the central sterile department are grouped into six functional areas:
- Decontamination
- Sterilization
- Transportation
- Emergency crash cart stocking
- Dental decontamination/sterilization
- Operating room
To be able to apply the model, the department also had to identify all the major activities performed in each of these functional areas. These activities had to be measurable in terms of quantity and time required to complete tasks.
For example, as shown in the exhibit below, in the decontamination functional area, two major activities performed are picking up soiled patient care equipment and surgical instruments and performing the decontamination process. Lincoln’s central sterile department uses a tracking system that captures the workload (e.g., number of pieces of soiled patient care equipment and soiled surgical instruments picked up on a daily basis) and total productivity time in the sterilization functional area. However, it does not capture the time associated with the pickup of these items, nor does it capture the time required to decontaminate each piece.

To determine the pickup time in the decontamination functional area, department staff implemented a log-in sheet where they documented their daily pickup time for a period of three weeks. They then conducted a time study in the decontamination area to determine the average time technicians took to decontaminate each piece.
Calculate weekly productive labor hours required for each functional area. With respect to weekly productive hours in the decontamination functional area, for example, the tracking system generated a weekly report that provided the total number of soiled pieces picked up over the week, as shown in the previous exhibit. Lincoln then multiplied the weekly average quantity of soiled patient care equipment by the average time it takes to decontaminate each piece of equipment to obtain weekly productive hours required for this purpose, with this process repeated for soiled instrumentation trays. The same process was applied to all other functional areas, with the exception of sterilization.
For the sterilization functional area, the tracking system generated a report showing the total productive hours utilized over the course of a year. Lincoln then divided the total annual productive labor hours by 52 weeks to obtain the weekly productive labor hours required.
Determine the number of FTEs required annually. Based on the weekly productive hours required for each functional area, the annual FTEs needed for the central sterilization were calculated, as shown in the exhibit below.
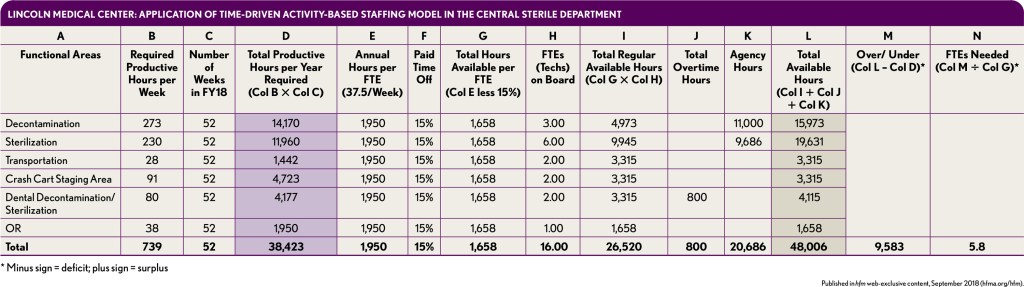
The time-driven activity-based staffing model demonstrated that, contrary to anecdotal reports, there were considerable opportunities for improving productivity in the central sterile department, and the current weekly productivity of the department could be accomplished in 12 scheduled shifts rather than the 21 scheduled shifts that previously had been deemed necessary. With the implementation of this staffing model, Lincoln reduced its staffing needs by six FTEs and eliminated nine shifts per week with their associated costs.
Case Study No. 2: Trauma Center
Lincoln Medical Center’s Level 1 trauma center includes one of the busiest emergency departments (EDs) in the country. The hospital’s CEO underscored that the hospital had an urgent need to streamline its ED registration process as an up-front means to prevent revenue leakage from denials and registration errors.
As part of the hospital’s action plan, the CFO and the CNE sought to measure the ED unit clerks’ productivity to determine whether additional resources were needed to capture all ED patient registrations and minimize denials. Because the CFO and CNE are responsible for the registration clerks and the unit clerks respectively, the two leaders decided to deploy a repurposed TDABC approach to measure the productivity of each of these staffing categories.
The two staffing analyses disclosed that productivity of the ED unit clerks was at 63 percent, compared with 91 percent for the registration clerks. It also became apparent that productivity of the two groups could almost be evened out simply by transferring two functions of the ED registration clerks to the ED unit clerks—namely e-prescribe enrollment and completion of regulatory forms. The productivity scenario analyses also persuaded the leadership not to hire additional resources. Rather, the leaders agreed to restructure the functions and responsibilities of the staff to optimize the registration process.
Key Takeaways
These two case examples demonstrate the potential benefits to be gained from creatively implementing the principles of TDABC methodology to optimize existing resources. At Lincoln, the activity-based staffing model has been wholly accepted by clinical, operational, financial, and administrative leaders as a valid and reliable tool for strategic planning and has been deployed in many other ways than those describe here to improve the cost effectiveness of hospital operations.
The message from Lincoln’s experience is clear: Any hospital or health system that creatively applies TDABC principles across all areas of its organization can effectively optimize its services, realize cost savings, and ultimately improve its overall efficiencies and effectiveness. Conducting the productivity analyses required for such an undertaking invariably takes time and resources, but the benefits in terms of overall operational improvements make the effort well worthwhile. At Lincoln, inventively repurposing TDABC principles has provided management with a value-added tool—one warranting the attention the other healthcare leaders, who then should focus on learning and using the methodology to improve the competitive positions of their institutions.
Sourjya Patnaik, MBA, CHFP, is director of nursing financial operations, Lincoln Hospital, Bronx, N.Y., and a member of HFMA’s Metropolitan Chapter of New York.
Lillian Diaz, RN, MBA, is chief nursing executive, Lincoln Hospital, Bronx, N.Y.