





Contracting
White House zooms in on hospital contracts
The issue's framing as a healthcare affordability issue may spur more legal challenges from anti-trust agencies.
Published
June 30, 2026
10:19 am
The Trump administration is tightening scrutiny of provisions of contracts of hospitals with payers, which could spur additional lawsuits or legislation, say attorneys.
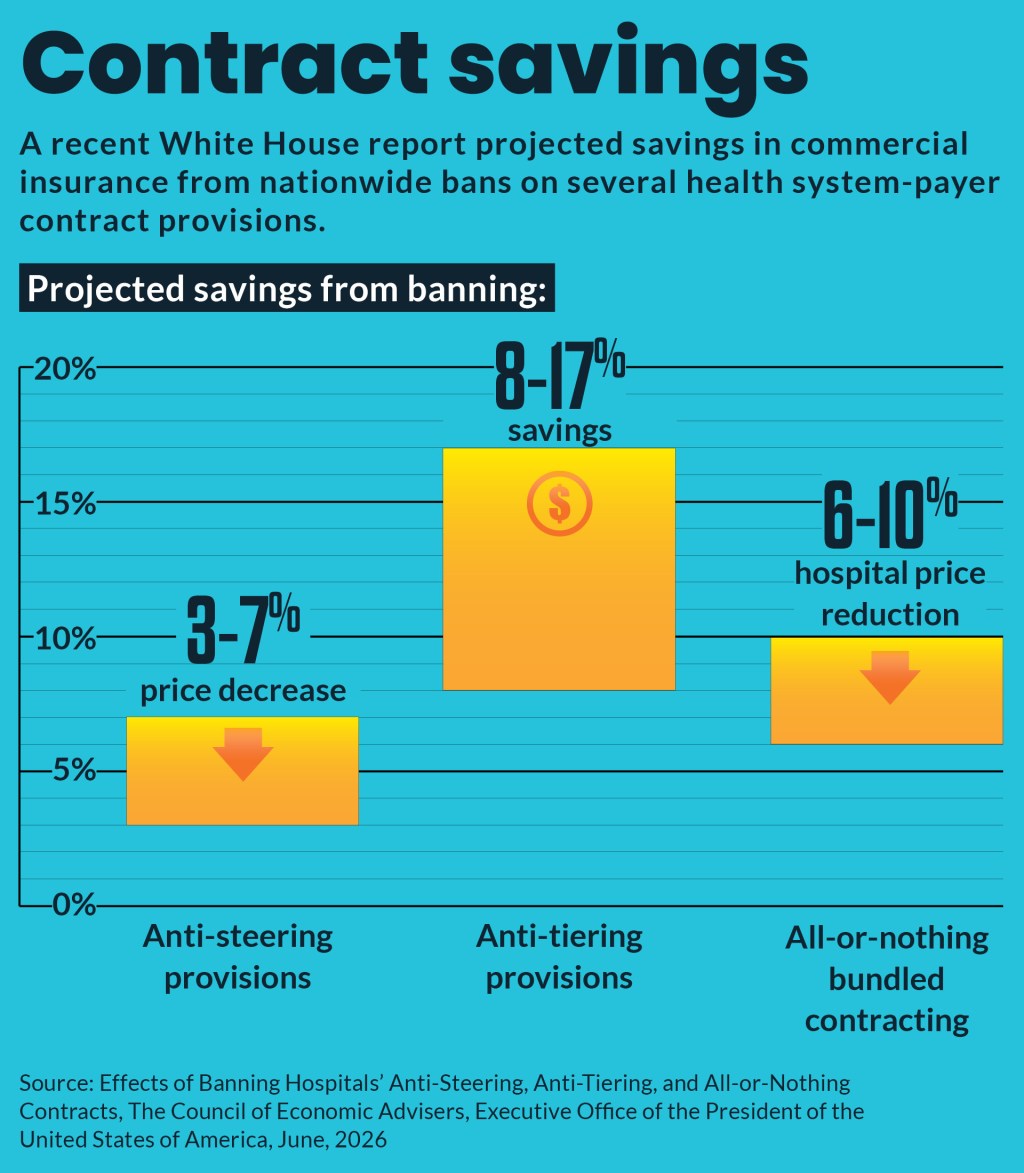
The White House Council of Economic Advisers issued a June 18 memo laying out its case against health systems’ use of several contract provisions focused on:
- Anti-steering, which prevents payers from offering patients financial incentives to choose lower-cost providers
- Anti-tiering, which requires payers to place the system in the most favorable cost-sharing tier regardless of price
- All-or-nothing, which requires payers to include all of a system’s hospitals and affiliated physicians in network or none at all
The memo couched a nationwide ban on such provisions as a healthcare affordability measure with projected benefits that include:
- 11% to 26% cut in hospital and affiliated-physician prices
- 4% to 7% cut in employer-sponsored insurance (ESI) premiums
- $1,100 to $2,500 per family annual savings or wage increases
- $29 billion to $63 billion annual nationwide savings across all ESI populations
The memo referenced the Department of Justice’s (DOJ’s) ongoing lawsuit against use of such provisions by NewYork-Presbyterian. The DOJ also recently settled a suit against OhioHealth’s use of those contracting provisions. Per the settlement, OhioHealth cannot implement anti-steering or anti-tiering clauses, nor use provisions that stymie price transparency.
Why it matters
The White House memo indicated to legal observers that the targeted contract provisions are seen as increasingly important to federal officials.
The memo “underscores that the administration as a whole, beyond just the DOJ, is focused upon these contract provisions,” David Gonen, a partner at the law firm Katten Muchin Rosenman, said in an interview.
Zachary Johns, an antitrust partner at Morgan, Lewis & Bockius, described the White House memo as “a very bold proposal” that may lead to federal legislation. But in the short term, it likely will inspire more legal action.
“You could see the antitrust agencies saying, ‘Well, OK, now we need to do more here because this is something that has been underlined as having direct dollar savings to employers, small businesses, patients, consumers, and it affects everybody, a huge segment of the economy,’” Johns said in an interview.
The attorneys were unaware of existing legislation focusing on health system contracting provisions, but such bills advanced in 2023 in the Senate and in 2024 in the House of Representatives.
Legal targets
The federal lawsuit push against such contract provisions started about 10 years ago when the DOJ sued Atrium Health over such language in its payer contracts.
The latest cases were significant in that they demonstrated that federal antitrust enforcers are willing to target the contract provisions of health systems with smaller market shares. The targeted health systems in previous lawsuits held majority market shares in their markets but NewYork-Presbyterian had as little as a 25% market share, depending on the geographic market measured.
Gonen said health systems with less than a 20% market share still are less likely to face DOJ scrutiny for the use of such contract provisions.
“It’s larger hospital systems that are more likely to be scrutinized. For providers whose share is above 25% or 30% in a given market or where it’s dominant or where it’s the only hospital in a certain market, these clauses require careful consideration,” Gonen said.
Health systems also have faced an increasing number of private class actions against such contract provisions, which carry large potential monetary penalties. That financial vulnerability was demonstrated in the $228.5 million settlement last year in a civil class action against Sutter Health, which stemmed from a previously settled state antitrust enforcement case.
Defensive moves
Health systems can at least take steps to prepare for increased legal scrutiny.
If payers are requesting such contract provisions, as NewYork Presbyterian stated in its response to DOJ’s complaint, health systems should document that at the time of the negotiations, said Gonen.
Documentation also was underscored by Johns, who noted that finance staff involved in negotiations need to ensure that written communications about negotiations reflect how they would benefit patients.
“You want to always be thinking about how what I am asking for benefits the patients and allows me to deliver more efficient and superior care,” Johns said. “And if you have that North Star, as I know almost every health system does, you document how what you’re asking for allows you to do that.”
Johns suggested that health systems review the proposed final judgment with OhioHealth, which identifies the types of anti-steering provisions and gag clauses that DOJ wanted disallowed.
“If I were in a health system, I would be turning around and saying, ‘Are we doing something that’s like this, because this is what the DOJ is most focused on,’” said Johns. “And I would want to get a handle on, if we’re using that stuff, No. 1, that it’s exactly like this, or two, could it be close to it?”
Payer response
The White House memo may embolden payers to more forcefully challenge all-or-nothing arrangements, which frequently is an agreement ahead of and separate from the contract.
“You might see payers a little bit more emboldened to try to break apart your network, and say, ‘Look, these hospitals over here on the western side of the state or the eastern side, the ones that are sort of far away, we don’t really need those for this population center that we’re primarily focused on,’” Johns said.
In such cases, health systems could push back with valid business arguments, such as administrative simplification for their facilities in dealing with a single contract; that a unified contract helps support high-quality patient care; and various harms from lacking it, such as preventing care for certain patient populations.
“But as long as they’re documented in the right way, that’s really the key,” Johns said. “The overall takeaway from all of this is your documentation in real time is so important.”