





HFMA Enterprise memberships drive engagement, retention, independent study finds

Organizational memberships drive employee engagement, provide clear career development paths and reduce turnover, according to results published in an independent study commissioned by HFMA. Adding to the benefits of association organizational memberships that offer training and education versus a similar individual membership are the cost savings of buying in bulk, which can reduce training costs by as much as 80%.
The study results were summarized in a white paper, An independent assessment of association organizational membership for healthcare organizations, which was developed by the research company Association Insights, Smyrna, Georgia.
“The significant benefit of organizational membership is a stronger career foundation for employees, rooted in continuing and advancing career expertise and recognition,” the report states. “Organizational membership provides a structure for career advancement within healthcare finance through certifications.”
“One example of the effectiveness of this membership model is HFMA’s Enterprise Solutions program, introduced in 2018, when membership hovered around 40,000,” said Bill Casey, senior vice president of membership experience for HFMA. “In April, the Association’s 100,000th member joined the program, attesting to its appeal.”

Today, many of the organizations Casey speaks with are incorporating HFMA’s certification courses into the career paths established for employees.
“Especially during the pandemic, organizations were looking for solutions to build revenue cycle competencies among their teams,” Casey said. “What we’re finding is Enterprise members are highly engaged within their cohorts in our HFMA communities. This expands their knowledge, extending the benefits of membership beyond programs and certification.”
9 benefits of organizational memberships

In light of the ongoing healthcare workforce issues, such as difficulty in retaining and recruiting both clinical and administrative employees, the study results are promising, said Rich Lucas, HFMA’s director of member channel assets.
The study found nine key benefits of organizational memberships:
- Creating gateways to employee career development
- Increasing employee engagement
- Enhancing the overall value of membership
- Reducing cost per employee member
- Developing consistency in work processes and improved quality
- Elevating the overall level of employee education
- Supporting employee recruitment efforts
- Raising employee retention (survey respondents reported staff retention increases of 20%)
- Improving employee performance
“The tangible benefits of the program underscore the value of this type of membership for organizations,” Lucas said.
Study methodology
The results of this independent study are based on two online surveys of 77 HFMA Enterprise member organizations’ program administrators (43 participants) and executives (34 participants), along with in-depth telephone interviews with three program executives representing Enterprise member organizations. The researchers also incorporated data from HFMA’s regular monthly and quarterly surveys of Enterprise members. The study was commissioned by HFMA to gauge how organizational memberships benefit organizations, using HFMA Enterprise membership as an example.
“We’ve seen the growth of our Enterprise Solutions organizational membership program over the past five years and heard about the value from members, but for full transparency, we wanted a third party to conduct the research and author the report,” said Lucas.
For more information
For full insight into the study results, download the white paper, An independent assessment of association organizational membership for healthcare organizations.
Is Your Organization Maximizing HCF Funding—and Fully Prepared for an Audit?
The Healthcare Connect Fund (HCF) represents one of the most significant funding opportunities available to healthcare organizations today—yet many systems fail to capture its full value. Between complex eligibility requirements, evolving infrastructure, and strict compliance standards, it’s easy to overlook critical opportunities or introduce audit risk.
This Healthcare Connect Fund Audit Readiness & Funding Strategy Scorecard is designed to help healthcare finance and IT leaders quickly evaluate where they stand. From eligibility validation and competitive bidding to documentation management and reimbursement tracking, the scorecard provides a structured framework to assess both funding performance and compliance posture.
HCF offers up to 65% reimbursement on eligible services, including connectivity, equipment, and network infrastructure. However, participation requires more than just filing—it demands ongoing strategy, disciplined documentation, and audit readiness. As highlighted in the scorecard, audits are guaranteed—not occasional—making proactive compliance essential to protecting funding and avoiding costly findings.
Organizations that lack a defined funding strategy or audit readiness process often face delayed approvals, missed reimbursements, and increased administrative burden. In contrast, those with a proactive, data-driven approach are able to maximize reimbursement, strengthen compliance, and drive long-term financial value.
Use this scorecard to identify gaps, benchmark your current approach, and determine whether your organization is fully positioned to capture every available dollar—while remaining audit-ready at all times.
Download this white paper to:

- Evaluate your organization’s HCF funding strategy and audit readiness
- Identify missed reimbursement opportunities across eligible services
- Strengthen compliance processes to reduce audit risk
- Validate eligibility across all healthcare sites and consortium structures
- Improve documentation practices to support audit defense
- Optimize funding performance through a more strategic, proactive approach
- Benchmark your current filer or internal process against best practices
- Take actionable steps to maximize financial outcomes from HCF
HFMA recognizes leaders for advancing Enterprise engagement
HFMA’s Enterprise membership empowers healthcare organizations with practical resources and relevant education to cultivate their finance teams. Since Enterprise Solutions was introduced in 2018, HFMA’s Enterprise membership has grown exponentially.
While HFMA works closely with Enterprise partners to design customized programs, internal Enterprise leads work to promote these resources. Now, these unsung heroes are finally getting the recognition they deserve through the Enterprise Impact Award, established in 2025 to honor individuals who champion HFMA engagement across their organizations.
“Although Enterprise leads work behind the scenes to connect their teams with HFMA resources, they directly influence how employees grow and engage within their field,” said Craig Nesta, one of the winners who will be recognized at the upcoming HFMA Leadership Summit, April 26-28 in Austin, Texas.
2025 HFMA Enterprise Impact Award winners
Here is a look at the 2025 Enterprise Impact Award winners and how they are strengthening their workforces through HFMA Enterprise membership.

Kevin Barron, vice president of payer relations at University Health. Barron enhanced Enterprise engagement at University Health by integrating HFMA membership benefits into departmental onboarding, performance planning and corporate strategy. Through continuous communication and a dedicated intranet hub, Barron amplified engagement across all operational areas of the organization. Within 18 months, HFMA membership at University Health expanded from one active member and four certifications to 219 active members and 63 certifications.

Jackie Chalarca, director of revenue integrity at Moffitt Cancer Center. Chalarca elevated HFMA participation as a cornerstone of Moffitt’s finance education strategy by embedding membership into the culture. Beyond encouraging attendance at local HFMA chapter events, Moffitt hosts its own annual education event with participation exceeding 230 attendees. Incorporating certifications into onboarding modules and advancement pathways helped expand participation to 1,374 employees across the clinical, research and administrative teams.

Nikki Harper, chair of revenue cycle – automation, analytics and diversified revenue at Mayo Clinic. Harper created a comprehensive communication strategy that highlights HFMA resources and celebrates individual achievements to showcase the value of membership. Her structured campaigns increased elearning utilization by 50%, boosted webinar registrations and attendance at 656 events in 2025, supporting 488 certified professionals across the organization. Harper also encouraged extensive chapter involvement, resulting in 16 chapter committee roles and five national HFMA leadership roles filled by Mayo staff.

Craig Nesta, vice president of Emerson Practice Associates at Emerson Health. Nesta elevated HFMA chapter involvement by integrating professional networking, volunteer leadership and career development into Emerson’s workforce strategy. He reinforced Emerson’s commitment to professional growth by promoting enterprise membership in monthly meetings and recruiting events, while recognizing employees through social media and internal communications for their involvement.

Hannah Perez, manager of revenue cycle operations at Corewell Health. Perez strengthened engagement at Corewell Health through constant communication and supportive outreach that made HFMA resources easily accessible. She coordinated a centralized hub, monthly email newsletters, and educational events — including a record-setting mentorship session that drew nearly 700 attendees. Her efforts grew HFMA membership within her organization from under 1,000 to 4,187 over five years, with 629 revenue cycle team members earning or maintaining certifications last year.

Chelsea Suschanke, director of revenue quality and performance improvement at Phelps Health. Suschanke transformed HFMA engagement by embedding education and certification into departmental operations. Her leadership expanded HFMA participation from 13 members to 268, increasing membership at Phelps Health by 57% in 2025. She designed custom learning dashboards aligned to specific revenue cycle roles, driving 112% growth in e-learning completions from 164 in 2024 to 347 in 2025. Her enterprisewide initiatives resulted in 33 new certifications last year.

Theresa Wagenman, CFO (formerly controller) at Grand River Hospital District. Wagenman expanded HFMA engagement within a rural critical access hospital by removing financial and educational barriers to create meaningful development opportunities for staff. By implementing certification incentive programs, Wagenman achieved approximately 75% staff engagement, with 55 members enrolled, 37 education courses completed and 13 certified employees.

In addition to these seven honorees, HFMA has an award for Mary Kirkendall, recognizing her individual efforts in promoting the benefits of HFMA membership. She has guided peers in effectively leveraging HFMA resources to drive meaningful outcomes, applying strategic planning and systematic processes to address both operational and individual needs.
How to participate in next year’s awards
Get ready to share your engagement strategies and successes by nominating your organization’s Enterprise lead when HFMA calls for applications in October 2026.
5 takeaways to drive enterprise engagement
The success stories of these winners of HFMA’s inaugural Enterprise Impact Award offer best practices to inspire Enterprise leads at other healthcare organizations. Try some of these tactics to engage your team:
- Embed HFMA participation, eLearning completion and certification into onboarding programs and performance goals.
- Develop centralized resource hubs and customized dashboards to create accountability and track progress.
- Communicate consistently across channels to spread awareness of HFMA programs and opportunities.
- Celebrate HFMA achievements to recognize employees and encourage participation.
- Promote chapter leadership and volunteer involvement as pathways to professional development.
Chapter partnership with OU drives student engagement
In just over two years, a partnership between the HFMA Oklahoma Chapter and the University of Oklahoma (OU) Hudson College of Public Health has not only enhanced students’ healthcare finance education but also helped 54 of those students earn the Certified Specialist in Payment and Reimbursement (CSPR) certification.
Bringing HFMA certifications to local university curriculum

In that time frame, OU student members of HFMA earned a total of 62 HFMA certifications, which included others besides CSPR available to them through their membership. Students enrolled in the OU MHA program are required to pass only HFMA’s CSPR certification exam, which is complementary to the university’s Managed Care and Integrated Systems course.
The course is taught by university lecturer Ann Paul, DrPH, MPH, who has required students pass the certification exam as part of the curriculum since the fall semester of 2023. The initiative is growing, with Paul’s colleague in the MHA program, Ganisher Davlyatov, PhD, requiring students to achieve Certified Revenue Cycle Representative (CRCR) certification as part of his course on health information systems this coming fall.
“Resources offered by organizations such as HFMA are integral to student education because much of what we do in healthcare relies upon understanding the finance side,” said Paul, a retired healthcare executive who has been an HFMA member since 1995.
Securing HFMA chapter resources

Paul connected with Chapter leadership on ways to have students join HFMA so they could complete the certification and asked for financial support because the school has a policy of not paying for this type of membership. The cost per student membership is $50.
Tyler Bernier, FHFMA, CPA, partner, Eide Bailly LLP, Oklahoma City, and an Oklahoma Chapter Committee Chair, said the Chapter was already having discussions about leveraging scholarships for student engagement when Paul’s request was received.
“This opportunity fit well with a concerted effort we were developing to improve student involvement with the Chapter,” said Bernier.
As the certification initiative evolves, the Chapter is seeking ways to increase student engagement with its activities and events. Current tactics under discussion include discounted or complimentary conference access for students, recognition opportunities and identification of individual student interests to increase involvement.
Automated payment reconciliation emerges as critical gap in healthcare revenue cycle
Despite strong integration and automation across patient care and general financial systems, healthcare providers still face a significant blind spot in banking integration — one that continues to cost time and money. According to a Wells Fargo survey conducted by HFMA, fully automated reconciliation remains out of reach for many organizations.
The survey, conducted in September 2025, focused on reconciliation practices, pain points and strategic opportunities for improvement. It also highlighted the reconciliation challenges organizations of varying sizes face, including staffing hurdles at small organizations and data inconsistency within mid-sized and large entities.
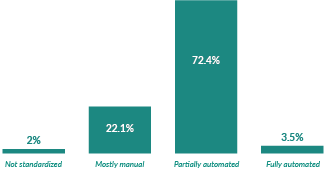
The survey recorded responses from 241 healthcare executives or directors from hospitals (51%), health systems (38%) and medical groups (11%). While automation has advanced in areas like accounting, operations, finance and patient financial services (PFS), revenue cycle processes continue to lag, with over 41% of healthcare organizations still relying primarily on manual workflows.
Digging deeper, 72% of respondents shared that their payment reconciliation processes are only partially automated, while more than 22% still rely on mostly manual workflows for reconciliation. Just 3.5% of respondents reported that their reconciliation processes were completely automated. This demonstrates a significant gap and a major opportunity for transformation, according to Tyler Siegfreid, CRCR, MHA, executive director of healthcare product management for Wells Fargo.
“What I found most surprising from the survey is how little integration these organizations have with their banks,” Siegfreid said. “This is a missed opportunity to experience bottom line value.”
Reconciliation processes mostly characterized by partial automation
How would you describe your organization’s current reconciliation process across the revenue cycle?
Integration is critical among EHR, ERP and banking systems
Overall, 77% of healthcare organizations represented in the survey report at least partial three-way reconciliation among electronic health records (EHRs), enterprise resource planning (ERP) and banking systems, which can reduce manual processes and errors while improving overall operations. While ERPs support a wide range of functions, the general ledger (GL) remains the core financial record, underscoring the need for tighter alignment between these systems.
The level of integration depends on an organization’s size, with 23.5% of the largest healthcare organizations reporting full integration, compared with just 3% of those with less than $500 million revenue. However, across participants, partial or full integration hovers around 70% for accounting, revenue cycle administration/operations and revenue integrity. Higher levels of integration are seen in finance (77.3%) and PFS (86.8%).
Not surprisingly, respondents from organizations of all sizes point to the EHR as being the most critical technology to their reconciliation efforts. They also believe that seamless three-way integration (EHR, ERP and banking systems) should be a priority, with 46.5% expressing that sentiment, ranking above end-to-end automation of reconciliation workflows (26.4%), advanced analytics and real-time dashboards (14.6%) and staff training/process standardization (10.4%). Results were consistent across financial processes and organization size.
Payment posting and reconciliation to an EHR represents the largest reconciliation challenge, cited by 44.4% of survey respondents. It was also the top challenge across finance departments and by organization size, defined by net patient revenue. Other challenges mentioned include bank matching and treasury controls (14%), ERP reconciliation (12.9%) and patient payment collections (15.8%).
A standardized Bank Administration Institute (BAI) file from a financial institution can reduce manual processes by sending data directly to an ERP or GL system.
“Obviously, revenue cycle and finance are the main departments dealing with this, but so are PFS, clinical departments and non-patient services teams — everything from the cafeteria and gift shop to the parking garage,” Siegfreid said. “Cash management is incredibly complex, but there are ways to make it easier and reduce frustration for financial teams, such as by eliminating the use of spreadsheets and the need to manually key in data through automated bank data file integration.”
Reconciliation pain points and workarounds
When asked about their biggest reconciliation pain point, over one-third of respondents noted data inconsistencies across systems and vendors. Staffing limitations and the cost of dedicated reconciliation teams followed at 31.4%, with lack of real-time visibility close behind at 20%. This is one area where organization size made a difference, with 40% of the smallest companies pointing to staffing issues as their primary pain point, while the largest organizations struggled most with data inconsistency.
Staffing issues at smaller organizations play a role in how reconciliation errors occur, with nearly 36% reporting issues with manual data entry and postings. In contrast, larger organizations unanimously pointed to complex contracts and varying reimbursement rules as the top reason for errors. And when it comes to resolving discrepancies, providers with under $10 billion in revenue primarily use manual adjustments, while the largest providers rely on vendor platforms or third-party reconciliation solutions.
“Regardless of whether a provider is a three-physician clinic or a 200-bed hospital, they have to do the same financial activities, but with a different level of revenue, technology and staff to do it,” Siegfreid said. “There is a misperception that small organizations will not greatly benefit from reconciliation. However, we see organizations of all sizes experiencing efficiency gains they couldn’t have forecasted. In other words, automating reconciliation opens the door to increased efficiency and reduced cost for healthcare organizations of all sizes.”
Despite hiccups, confidence in financial data is strong
Reconciliation errors reverberate throughout organizations and can impact financial operations and strategic decision-making. However, only 10% of companies say those impacts are significant, with 43% indicating only occasional impact and the rest reporting rare or minimal impact on operations.
Likewise, confidence is high across organizations in their ability to maintain accurate and timely reconciliation across systems. Nearly nine out of 10 respondents expressed moderate or high confidence in their reconciliation processes. The largest organizations were 100% confident, while organizations in the other revenue tiers reported 85% confidence.
“There is a lot of opportunity for more automation and integration in healthcare from a reconciliation and revenue cycle perspective,” Siegfreid said. “The survey underscores the importance of the EHR to this process, but it also points to the need for tight integration with financial institutions to provide a record of truth that can reduce errors and improve reconciliation efforts.”
Conclusion
Organizations of all sizes are actively working to improve processes through increased automation, but each market segment has its own challenges. Smaller providers struggle with staffing and resource challenges that perpetuate manual data entry and reconciliation, while larger organizations note data discrepancies and integration gaps among technologies. The largest providers are in the best shape to strengthen reconciliation, technology-wise, but integration challenges still prevent full automation.
About Wells Fargo & Company
Wells Fargo & Company (NYSE: WFC) is a leading financial services company that has approximately $2.1 trillion in assets. We provide a diversified set of banking, investment and mortgage products and services, as well as consumer and commercial finance, through our four reportable operating segments: Consumer Banking and Lending, Commercial Banking, Corporate and Investment Banking, and Wealth & Investment Management. Wells Fargo ranked No. 33 on Fortune’s 2025 rankings of America’s largest corporations. News, insights, and perspectives from Wells Fargo are also available at stories.wf.com. Additional information may be found at wellsfargo.com.
This published piece is provided solely for informational purposes. HFMA does not endorse the published material or warrant or guarantee its accuracy. The statements and opinions by participants are those of the participants and not those of HFMA. References to commercial manufacturers, vendors, products, or services that may appear do not constitute endorsements by HFMA.
RCM recalibration: Patient financial experience captures leaders’ top focus
Healthcare finance leaders constantly navigate pressures to sustain growth, control costs and improve efficiency to enhance revenue cycle management (RCM). As technologies advance, patient expectations evolve and reimbursement rates remain elusive, these uncertainties make the balancing act even more precarious.
A recent survey shows that healthcare finance leaders are shifting their priorities and investment strategies to stay ahead of these challenges.
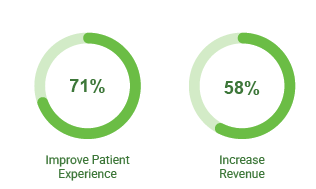
According to FinThrive’s third-annual Transformative Trends and Data-Driven Insights Report, 2025 signaled a structural recalibration in how healthcare leaders define financial performance. For the first time since FinThrive began conducting this survey, patient experience surpassed revenue growth as the top strategic priority among revenue cycle leaders, with 71% of executives ranking it as their most important goal.
This shift reflects a growing recognition that revenue growth is increasingly achieved through experience-driven operational design which drives patient loyalty over traditional volume-based strategies. In fact, the top-performing organizations recognize that these two priorities are intertwined, because better experiences attract and retain more patients, protect market share, reduce friction and stabilize margins over time.
“Patient experience is a revenue growth goal,” said Jacob Collins, vice president of revenue cycle at Phoebe Putney Health System in Southwest Georgia. “In other words, experience doesn’t replace revenue; it’s how you obtain it.”
Instead of choosing between patient experience and economics, leaders are increasingly relying on AI, automation and integration to reduce friction across the revenue cycle — leveraging technology to combat denials, streamline authorizations, improve documentation and enhance every other touchpoint along the way.
Survey results also reveal how healthcare finance leaders are connecting patient loyalty, RCM efficiency and automation into one cohesive strategy for operational resilience.
Workflow reality check
Until recently, many health leaders assumed that the patient experience referred only to clinical care. But increasingly, organizations understand that it’s the entire experience — not just great clinical care, but a smooth onboard to the organization, correct and timely data capture and convenient ways to pay — that distinguishes them, according to Collins.
“Healthcare is complex, and there are a lot of different touchpoints throughout the revenue cycle between scheduling, authorization, eligibility and financial clearance that can create ‘interaction fatigue,’” Collins said. “Reducing the friction can help improve that experience.”
The interaction fatigue of manual revenue cycle workflows can frustrate patients who face delays or redundant payer approval challenges; and it can also wear on staff, who are prone to burnout and even leave because of the heavy administrative burden. Each point of friction carries financial implications as patient and staff attrition leads to revenue leakage, slow cash flow and strained resources — triggering a spiral of poor financial performance.
Fortunately, innovative technologies offer effective solutions to smooth these workflows and improve the experience for patients and staff alike. Not surprisingly, automation and AI adoption is surging among health finance leaders, with three out of four citing automation as a top initiative for 2026 and more than half (56%) reporting AI/automation as their prime investment focus.
Patient experience takes the lead
71% of financial leaders rank it as their top focus, compared to 58% who chose revenue growth.
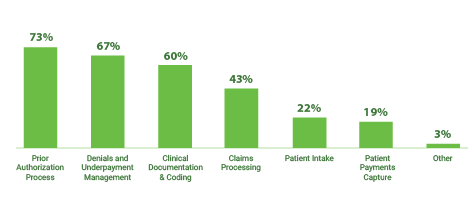
The top three use cases for RCM automation focus on streamlining these bottlenecks by targeting the prior authorization process (73%), denials and underpayment management (67%) and clinical documentation and coding (60%).
“We’re implementing targeted, smart, efficient automation and AI capabilities,” Collins said. “That does two things: One, it helps control expenses in terms of the resource component, and two, it allows our team to focus on more complex issues and patient-centered interactions.”
Likewise, nearly six out of 10 leaders surveyed agreed that the primary driver behind AI investment is alleviating administrative burdens, with the goal of minimizing errors and turnaround times while freeing staff for more important work.
In fact, Collins said, the biggest risks of dismissing revenue cycle automation are staff burnout and turnover.
“As leaders, we need to take care of our staff by giving them the tools to do their jobs more efficiently,” he said, “and process automation is one of the tools you can use to make their jobs easier.”
After all, the same manual tasks that drain staff also degrade patient experience, which will ultimately deplete the bottom line.
“If I’m not automating my front-end processes, my patient access team is not going to have the most effective tools. If they don’t have the most effective tools, then patient experience is going to decline, and people are going to go where it’s easier to get in, where authorizations are coming more quickly and estimates are more accurate, where there is less friction,” Collins said. “As those front-end processes bottleneck, your revenue on the backend is going to decrease.”
Where do healthcare finance leaders believe AI and automation will have the most significant impact?
AI and automation will most significantly impact:
Targeted investments
As part of healthcare’s RCM recalibration, organizations are redefining technology’s role in the revenue cycle. The survey results show leaders stepping back from short-term fixes like cost cutting — which ranked lowest among this year’s strategic goals at 36% — to focus instead on strategic technology investments that drive growth.
According to a separate study from FinThrive and HFMA, nearly half (47%) of healthcare organizations have already implemented multiple AI or automation tools, while another 38% are in early pilot stages. Given the vital role that technology plays in enhancing patient experience and boosting the bottom line, deciding where and how to apply technology represents a challenging decision.
“We’re always looking to cut costs and be more efficient where we can so we can continue to reinvest in our teams so that we can provide the best patient experience possible,” said Miguel “Mike” Vigo IV, chief revenue cycle officer at UC San Diego Health in California. “When it comes to AI, we’re very meticulous in how we’re balancing our technology investments to add efficiencies, so we can grow organically without increasing costs.”
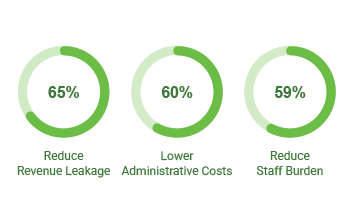
The Transformative Trends report revealed the top motivations for investing in automation, which include reducing revenue leakage (65%), lowering administrative costs (60%) and reducing the burden on staff (59%). For organizations like UC San Diego Health, tech investment decisions often consider all three of these factors simultaneously.
As organizations reassess their technology strategies, many are seeking clearer benchmarks to evaluate maturity and identify gaps across the revenue cycle. One approach that Vigo, like hundreds of other finance leaders, is using to bring structure to that assessment is the Revenue Cycle Management Technology Adoption Model (RCMTAM) developed by FinThrive in partnership with HFMA.[1] The framework leverages extensive benchmarking data — more than 30,000 data points — from healthcare finance leaders to help organizations benchmark their tech stack maturity, pinpoint gaps and prioritize opportunities where AI-enabled technologies can drive measurable improvements.
“The RCMTAM tool provided us with the clarity and direction we needed to either improve our metrics considerably or maintain transparency on stable KPIs,” Vigo said. “It’s been invaluable in helping us pivot resources and realign strategies.”
Of the several hundred RCMTAM surveys that have been completed, at least half of them have identified patient access as a potential gap, estimates Hemant Goel, president and CEO at FinThrive.
“That tells me the industry is somewhat immature on the front-end, and there’s an opportunity to modernize the patient experience,” he said.
The Transformative Trends survey confirms this observation, revealing that hospitals are investing in patient experience initiatives that influence financial outcomes — such as enhancing scheduling and self-service tools (52%) and improving payment processes (41%). Digital conveniences like these are no longer a competitive advantage; they are table stakes. Healthcare consumers demand seamless scheduling and flexible payment options, delivered with the same ease they experience in retail environments.
Health systems that meet these expectations see measurable gains not only in patient experience scores, but also in downstream financial stability. Failing to weigh the importance of the patient experience and focusing solely on revenue when making tech investments can deter success, puts health systems at risk, destroying both patient volumes and profit margins, Vigo said.
“If you deprioritize the patient experience, you’ll start to see your volumes decrease and then all of a sudden, your market share will drop as people reschedule to other places,” he said. “You have to be very methodical with your technology investments to make sure they benefit both your revenue and your patient experience.”
Top motivations for automation investment
Technology transformation
Looking ahead, the organizations that thrive will be those that focus on a combination of clinical and financial pathways for their patients, Goel said. This is best supported by connecting operational efficiency, patient loyalty and intelligent technology applications into a cohesive strategy, recognizing that long-term financial stability relies on a seamless experience.
For example, a collaborative and cohesive approach leverages technology to strengthen patient experience. Such an approach enables hospital employees to use intelligent tools that effectively and efficiently address potential issues for patients, deepening patient loyalty while strengthening financial outcomes.
Successful transformations require deliberate alignment across people, processes and technology along with a strategic approach that seeks to deploy the innovative benefits of an RCM platform over time, according to Collins.
“You don’t have to go ‘all in’ immediately,” Collins said. “You can take incremental steps and do some simple process automations to make your employees’ lives better, and that’s the key. A happy, effective workforce helps improve your patient experience and ensures patient loyalty.”
Incremental progress is practical, but success will depend on ensuring each investment reinforces a cohesive operating model. Leading organizations eliminate friction from the revenue cycle in an automated way, recognizing that patient experience, workforce sustainability and resilient technology should function as one integrated financial strategy.
“It’s time to take inventory of your current capabilities, and the RCMTAM is one way to do that,” Goel said. “There’s a ton of friction in the revenue cycle, and technology plays a role in removing that friction to enable it to run smoothly. You must have the people, processes and technology in place to wrap your arms around the patient financially as well as clinically.”
Even the most sophisticated automated workflows are only as reliable as the security protocols protecting them. Amid rising cyber risks, tech-savvy leaders are realizing that revenue cycle stability and data security are now inseparable.
According to FinThrive’s Transformative Trends and Data-Driven Insights Report, 85% of organizations have already modified their RCM technology strategies to protect against cybersecurity threats and clearinghouse interruptions.
“Never have I been as concerned about security and compliance as I am now,” said Collins. “Automated processes are only going to work if they’re built in a system that’s secure, so it’s imperative that not only my internal systems but also my vendor partners maintain vigilance around data security.”
As catastrophic cyber events across the industry have demonstrated, a single ransomware attack or system outage can completely halt insurance verification, authorizations, claim submissions and eligibility checks — seriously disrupting cash flow throughout the revenue cycle.
“If you can’t recover and send out claims quickly, the money will take months to come back,” said Goel. “And if you don’t have the cash reserves to endure the outage, that can be devastating to your profitability.”
In addition to an internal security team that ensures strict compliance with industry standards and certifications such as SOC, NIST, CSF and HITRUST, standby claims and standby eligibility solutions provide hospitals with critical backup capabilities during unplanned revenue cycle interruptions.
“Cybersecurity threats are very sophisticated, so it’s not a matter of if, but when,” Goel said. “It comes down to recovery: How quickly can you get your systems back online and return to normal operations? That timing is critical. The more you are down, the more the revenue is at risk.”
As new tools have emerged to enhance every step of the revenue cycle, the solutions tend to stack up — adding complexities and duplications that present stumbling blocks to smooth technology integrations. In fact, FinThrive research reveals that the average hospital uses between 15 and 30 vendors just to manage various aspects of RCM.
“EHRs were never designed to submit bills or process payments,” Goel said, “so as they started incorporating things like prior authorization and insurance eligibility, third-party solutions had to bridge that gap between payer, hospital and patient. That has caused an explosion of RCM tools in the market.”
Now, as part of the RCM recalibration identified in FinThrive’s Transformative Trends and Data-Driven Insights Report, healthcare organizations are trying to reduce these complexities by consolidating vendors, with 71% planning to reduce vendors from their mix as they move toward a more unified RCM platform. This consolidation helps lower the cost to collect, simplify workflows, reduce risks and foster stronger accountability across the revenue cycle.
“There’s a lot of duplicity between RCM technology services, and the larger footprint you have, the more risk you have,” Goel said. “If everything’s all in one place, it’s a lot easier to understand how the eligibility transaction relates to the estimate, to the charges, to the bill, to the claim and ultimately to the payment. It becomes much more actionable to be alerted through analytics on one area versus going to 12 different places to collect those insights.”
This industry-wide shift toward vendor consolidation signals that organizations are looking for strategic, long-term partnerships with trusted vendors, rather than a patchwork of quick-fix point solutions. Organizations that seek to drive a lower cost to collect through effective financial pathways are well-positioned for financial sustainability for the future. The trends and initiatives identified in this survey drive toward that change and will enable improved financial outcomes for years to come.
About FinThrive
FinThrive delivers a comprehensive suite of revenue cycle solutions powered by a single, unified data foundation built for scale and intelligence. Organizations can adopt the RCM capabilities they need—from clearinghouse and claims management to denials prevention, patient engagement, insurance discovery, and analytics—while benefiting from shared data, embedded AI, and consistent workflows across the front, middle, and back of the revenue cycle. By replacing fragmented point solutions that limit visibility and drive costly inefficiencies, FinThrive enables revenue teams to unlock greater intelligence as adoption expands—where each added capability strengthens performance, accelerates cash velocity and predictability, and compounds financial value over time. Visit finthrive.com.
This published piece is provided solely for informational purposes. HFMA does not endorse the published material or warrant or guarantee its accuracy. The statements and opinions by participants are those of the participants and not those of HFMA. References to commercial manufacturers, vendors, products, or services that may appear do not constitute endorsements by HFMA.
Footnotes
[1]. Revenue Cycle Management Technology Adoption Model, FinThrive, www.finthrive.com/rcmtam.
FastFinance: Hospital non-patient revenue; ACA plan changes
HFMA’s FastFinance newsletter is now a podcast. Host Rich Daly discusses the most current and relevant healthcare news, delivered in an easily digestible format.
Most hospital revenue is from non-patient-care sources, according to a new analysis. The shares of patient-care revenue vary widely by hospital type.
Also, this week’s Weird Number: 40%. That’s the increase in bad debt and charity per calendar day when comparing year-to-date 2023 to year-to-date 2026.
One More Thing: Hospital advocates raised a range of concerns about proposed changes to ACA marketplace plan rules for 2027, including allowing more to purchase catastrophic plans.
Not a FastFinance subscriber? Learn more here.
News Briefs: Relief might be fleeting for healthcare after Supreme Court’s decision on tariffs
The Supreme Court’s Feb. 20 decision striking down most of the Trump administration’s tariff policy negated many of the tariffs that have affected healthcare and other industries since beginning in August 2025.
The ruling leaves in place sector-specific tariffs such as increased levies on imports of steel and aluminum, for which the tariff has been 50%. And in response to the decision, President Donald Trump immediately imposed a 15% global tariff via executive order, although any such tariff is statutorily limited to 150 days unless Congress approves an extension.
Trump also said he has long-term tariff options that would allow the administration to “charge much more” than previously. For healthcare, such an option could be in place when the temporary tariffs expire.
One path to legally implementing tariffs involves a formal investigation by the U.S. Commerce Department into an industry- or product-specific trade deficit. Such an investigation was launched in September and would have substantial implications for healthcare if the findings result in tariffs. The investigation is examining imports of personal protective equipment, medical consumables and medical equipment and devices.
CMS provides more leeway to Medicaid SDPs prior to new limits
A bulletin regarding Medicaid state-directed payments (SDPs) makes it easier for states to maintain eligibility for higher SDPs before the legislation known as the One Big Beautiful Bill Act (OBBBA) ushers in new restrictions starting in 2028.
That’s when existing SDPs must be reduced by 10% per year until reaching new caps of 110% of the Medicare rate in non-expansion states and 100% in expansion states. Those limits already apply to non-grandfathered SDPs, per the legislation. Before the OBBBA, the regulatory ceiling for hospital and skilled nursing facility SDPs was the average commercial rate.
According to the new guidance, SDP rates can be grandfathered and thus continue to exceed the new caps through 2027 if the SDP has a Medicaid rating period within 180 business days before or after the OBBBA’s enactment date of July 4, 2025. The new guidance supplants September 2025 guidance that set the time frame at 180 calendar days, rather than business days, meaning the revision gives states a larger window in which to capitalize on the grandfather option.
CMS proposes 2027 ACA marketplace changes to address rising premiums
CMS hopes the concepts published Feb. 11 in a proposed rule can help stabilize Affordable Care Act (ACA) marketplace plan enrollment from 2026 to 2027.
The proposals coincided with the Senate’s continuing inability to agree on extending the enhanced subsidies for the marketplaces, removing a key affordability mechanism in federally sponsored healthcare coverage.
The enrollment impact of allowing the subsidies to end remains to be seen. Through mid-January, reported enrollment was roughly 1.2 million lower than it was at the same point in 2025, with the potential for the gap to widen as enrollees who were auto-renewed drop out by choosing not to pay their initial premium.
Among other changes, the 2027 rule would make non-network plans eligible to join the marketplaces. Non-network plans do not maintain a contracted network of providers but would need to meet ACA standards for essential health benefits and coverage protections. They also would need to demonstrate that they offer a sufficient choice of providers, including those that furnish mental health and substance-use disorder services.
Hospitals urged to strengthen cybersecurity amid rising Iran-linked threats
Hospitals are among the organizations that should pay special attention to ensuring their cybersecurity is shored up amid the ongoing conflict in Iran, according to federal authorities.
Federal agencies and the American Hospital Association (AHA) have said they do not know of specific credible threats targeting U.S. healthcare. As a precaution, the FBI and the Cybersecurity Infrastructure Security Agency re-issued an alert that was published amid attacks by the United States on Iranian nuclear facilities in June 2025.
An attempted cyberattack by an Iran-aligned group may aim to disrupt service or steal sensitive data. Attacks may target not only clinical systems but also other components of hospital operations, such as patient portals or electronic health records.
During the week of March 9, the Michigan-based medical equipment manufacturer Stryker reported being hit by a cyberattack perpetrated by a hacking group linked to Iran. A company statement indicated that operations ranging from manufacturing to processing and shipping were affected.
Determining the MA payment rate for 2027
As published in January, the 2027 advance rate notice for Medicare Advantage (MA) health plans drew attention for keeping rates essentially flat relative to 2026. Here’s the estimated impact of the different components that affect the rate. CMS noted that the rate could change when the final notice is published in April.
| Element | Year-over-year rate impact |
|---|---|
| Effective growth rate | 4.97% |
| Rebasing/repricing | TBD |
| Change in star ratings | –0.03% |
| MA coding pattern adjustment | 0% |
| Risk model revision and normalization | –3.32% |
| Sources of diagnoses | –1.53%a |
| Expected average change | 0.09% |
Source: CMS fact sheet, “2027 Medicare Advantage and Part D advance notice,” Jan. 26, 2026
GAO examines No Surprises Act network patterns
Trends seen as a consequence of the No Surprises Act (NSA) include modest increases in the share of providers going in-network for emergency medicine and anesthesiology, according to a Government Accountability Office (GAO) report.
Increasing the availability of in-network providers was a secondary goal of the 2020 year-end legislation and could belie concerns that the large share of NSA arbitration decisions in favor of providers would diminish the incentive to join insurance networks.
Caveats to the findings include the indeterminate impact of additional factors, the GAO said, citing the COVID-19 pandemic and the increase in healthcare market consolidation during the five-year study period.
In addition, the agency said the findings apply only to the national and regional insurers that were included in the claims data set covering more than 110 million patients per year.
CMS details implementation of Medicaid 6-month eligibility checks
CMS has issued guidance on how Medicaid expansion states should implement the higher-frequency eligibility redeterminations as required under the One Big Beautiful Bill Act.
Starting in 2027, states must conduct eligibility checks of most adults in the expansion population every six months, up from annually under current policy.
The increased checks similarly apply to people covered under Section 1115 demonstrations that provide minimum essential coverage to all expansion adults in the state, CMS wrote in a March 6 bulletin.
The six-month requirement has raised concern for providers about an increase in coverage lapses among individuals who miss paperwork or do not respond on time. A recent RAND analysis projected that by 2034 the six-month checks will have led to a Medicaid enrollment reduction of 923,000.
People: 4 HFMA members move into new CFO roles
The first quarter of 2026 saw four HFMA members from various parts of the nation take on new CFO positions.
CommonSpirit welcomes Michael Browning as CFO

On Jan. 2, Michael Browning, MBA, CPA, began his tenure as the new system senior executive vice president and CFO for Chicago-based CommonSpirit Health. Browning is charged with financial oversight over the health system’s network of 138 hospitals and 2,200+ care locations across 24 states. In this role, he guides enterprise-wide financial planning and performance for the health system, overseeing accounting, treasury functions, reimbursement, revenue cycle operations, capital strategy and investor engagement. As part of his 30+ years of experience in healthcare finance, Browning has served as executive vice president and CFO at OhioHealth, having previously held senior leadership roles at several nonprofit health systems. He is a 22-year member of HFMA and a member of its Northwest Ohio Chapter.
Shelly Schorer expands her role to regional CFO for CommonSpirit

CommonSpirit Health appointed Shelly Schorer, FHFMA, MBA, as regional CFO for its South region, beginning March 1. The appointment follows her service of almost nine years as CFO of CommonSpirit’s California division. In her new role, her financial oversight will extend across markets in Arkansas, Kentucky, Ohio, Tennessee/North Georgia and Texas, encompassing the full spectrum of care. Schorer started her career in healthcare in 1998, and has held a number of other executive positions, including six years as Northern California division CFO for CommonSpirit Health and seven years as CFO for Mercy Health Joplin/Kansas. She has been an HFMA member since February 1999 and is currently a member of the Association’s Northern California Chapter.
Adam Smith moves into Mayo Clinic’s Wisconsin CFO position

Rochester, Minn.-based Mayo Clinic Health System has appointed Adam Smith, MSHA, CFO for its Wisconsin operations. Smith, who began his new role in January, oversees financial strategy, planning and operational performance across the state for the health system. Smith previously served for seven years, first as executive director and then as vice president, finance, for Milwaukee-based Froedtert Health, and prior to that, he served in various financial and operational leadership positions at the Medical College of Wisconsin. He joined HFMA in August 2018 and is a member of the board of directors for HFMA’s Wisconsin Chapter.
Powell Valley Healthcare taps Lisa Wooten to serve as its CFO

On Feb. 20, Lisa Wooten, MBA, began serving as CFO for Powell Valley Healthcare in Powell, Wyoming. Wooten provides financial oversight of the multifacility organization serving Wyoming’s Big Horn Basin, including a 25-bed hospital, a 100-bed long-term care facility and four medical office buildings. Wooten previously served for almost 11 years at Powell Valley Healthcare, first as director of materials and then as financial controller. Wooten joined HFMA in February 2025 as a member of the Wyoming Chapter.
To have your professional announcement published in People, contact Eric C. Reese at [email protected].
Ken Perez: AI, the healthcare industry’s private-sector-led revolution
With the advent of AI, many industry observers say the U.S. healthcare industry is standing at the brink of a sea change. As industrywide adoption of AI accelerates, now is a good time for the industry’s stakeholders to pause for a moment and take stock of what this new technology means for the healthcare system.
Remember the last time an emerging technology promised to revolutionize healthcare? It was 17 years ago.
In February 2009, in his address to a joint session of Congress, President Barack Obama stated, “Our recovery plan will invest in electronic health records and new technology that will reduce errors, bring down costs, ensure privacy and save lives.”a The recovery plan was the Health Information Technology for Economic and Clinical Health (HITECH) Act, which was enacted as part of the American Recovery and Reinvestment Act of 2009 (ARRA).
Federal government support for EHRs
Under HITECH, the federal government made available financial incentives to physicians and hospitals to adopt electronic health records (EHRs) and demonstrate their meaningful use. Initially, it was projected that this program would cost $27 billion over 10 years, but subsequent estimates pegged the cost much higher, with a 2019 article by Kaiser Health News and Fortune magazine reporting it as having reached $36 billion.b
Why did the federal government resort to this unprecedented way to motivate healthcare providers to adopt EHRs? With healthcare expenditures rising, it was thought that use of EHRs could improve the efficiency of the healthcare system, producing a so-called “digital dividend.”
Also, the United States lagged other industrial nations in adoption of EHRs. In 2008, while the United Kingdom, the Netherlands, Australia and New Zealand had nearly universal use of EHRs among general practitioners, only 10% to 30% of ambulatory care physicians in the United States and Canada used EHRs consistently.c Last, given the healthcare industry’s well-deserved reputation as a technology laggard — slow to adopt new practices, taking an average of 17 years for research evidence to change practice — it was felt that a strong “nudge” by the federal government, a combination of financial “carrots” (adoption subsidies) at first and “sticks” (penalties for non-meaningful use) later, was needed.d
The EHR incentive program’s results
HITECH achieved its basic goal of spurring EHR adoption. By 2017, 86% of office-based physicians had adopted EHRs and 96% of non-federal acute care hospitals had done so, according to the 2019 Kaiser Health News/Fortune article. However, there have been many downsides of EHRs, including the following.
Patient safety risks. Software glitches, user errors and other system flaws have resulted in medical errors in general and medication errors in particular.
Fraud. The software can be used to upcode, or overcharge, and some healthcare providers have allegedly overstated their use of EHRs, defrauding Medicare and Medicaid.
Lack of interoperability. David Blumenthal, Obama’s national coordinator for health information technology and one of the chief architects of the EHR initiative, acknowledged that interoperability goals took a backseat to just adopting one of the EHRs offered by more than 700 EHR vendors. As quoted in the Kaiser Health News/Fortune story, Blumenthal stated, “We had an expression: They had to operate before they could interoperate.”
Unfortunately, this, combined with perverse business incentives, resulted in EHR systems routinely being unable to talk to one another.
Physician burnout. The KFF Health News/Fortune article cites the findings of a 2017 study in the Annals of Family Medicine that physicians spend an average of 5.9 hours on EHRs compared with 5.1 hours spent with patients (out of an 11.4-hour workday).
Who won as a result of the EHR incentive program? Clearly, the largest EHR vendors benefited the most, prompting some to criticize the program as a huge wealth transfer from the American taxpayer to primarily those companies.
The promise of AI
Today, as AI similarly promises to revolutionize healthcare, the Trump Administration is cheering on this revolution. President Donald Trump opined in America’s AI Action Plan:
Today, a new frontier of scientific discovery lies before us, defined by transformative technologies such as artificial intelligence. .… Breakthroughs in these fields have the potential to reshape the global balance of power, spark entirely new industries, and revolutionize the way we live and work.e
In his former role as the director of the Digital Health Center of Excellence, Center for Devices and Radiological Health, in the U.S. Food and Drug Administration (FDA), Troy Tazbaz said:
Artificial intelligence .… is rapidly changing the health care industry and holds transformative potential. AI could significantly improve patient care and medical professional satisfaction. .… AI also has the potential to drive operational efficiency by enabling personalized treatments and streamlining health care processes.f
The Trump administration’s stance on AI for healthcare
However, in striking contrast with HITECH’s subsidization of EHR adoption, the Trump administration is not disbursing funds to healthcare providers to encourage them to adopt AI. This policy is partly due to two fiscal realities: CMS’s budget — which paid for the EHR incentives — is under pressure; and the Medicare Hospital Insurance Trust Fund is just eight years from insolvency.g
But more fundamentally, it reflects a philosophy of supporting private sector-led innovation, primarily by reducing burdensome regulations. To that end, as of December 2025, the FDA had approved 1,300 AI-enabled medical devices.h
Private sector investment in AI
The private sector’s AI leadership is evident, as it is pouring unprecedented amounts of money into AI. In 2026, Alphabet, Amazon, Meta and Microsoft — the so-called hyperscalers — are projected to spend $670 billion on AI infrastructure, more than 10 times the Apollo space program (1960-1973) as a percentage of the nation’s gross domestic product.i Healthcare, accounting for about a fifth of the U.S. economy, has emerged as the primary target of these investments. And digital health startups involving any AI component commanded valuation premiums and captured 62% of all venture funding in 2025.j
Healthcare’s adoption of AI
So, are hospitals using AI even in the absence of federal subsidies? The answer is, “Yes.” In 2024, 71% of hospitals reported using predictive AI integrated into their EHR.k And in terms of generative AI, according to a survey of 2,174 non-federal U.S. hospitals conducted in 2024, 31.5% reported using it and 24.7% planned to do so in one year. Thus, if the latter group of hospitals followed through in their plans, it would mean that by the end of 2025, half of non-federal hospitals in the U.S. were using generative AI.l
What lies ahead for AI in healthcare
These trends are certainly encouraging. But the jury is still out as to whether AI is delivering sufficient value to enable AI-focused digital health startups and other firms to evolve from surviving on venture funding to garnering substantive revenues and achieving profitability.
Reflecting on the heady nature of the current AI bubble, an AI leader at one of the hyperscalers recently told me that market consolidation is inevitable, which obviously would pose some risks for healthcare providers, such as unsupported software and outdated models and algorithms if AI vendors were to cease operations.
However, the value question and the inevitability of market consolidation are no different from what took place with EHRs. What is different is that the AI revolution is being led by the private sector, which incorporates the refining fire of market competition and dwarfs the size of the federal government. That means it has more staying power and greater prospects for success than the EHR incentive program ever had.
Footnotes
a. CMS, “Electronic health records at a glance,” July 13, 2010.
b. Worzala, C., “Policy update: Federal incentives for the adoption of electronic health records,” Journal of Oncology Practice, September 2009; and Schulte, F., and Fry, E., “Death by 1,000 clicks: Where electronic health records went wrong,” Kaiser Health News and Fortune,
March 18, 2019.
c. Jha, A., et al., “The use of health information technology in seven nations,” International Journal of Medical Informatics, December 2008.
d. Morris, Z., et al., “The answer is 17 years, what is the question: understanding time lags in translational research,” Journal of the Royal Society of Medicine, December 2011.
e. The White House, “Winning the race: America’s AI action plan,” July 2025.
f. Tazbaz, T., “Blog: The promise artificial intelligence holds for improving health care,” FDA, July 25, 2024; Tazbaz is currently senior vice president of corporate strategy & operations for Oracle in San Francisco.
g. Committee for a Responsible Federal Budget, “Social Security and Medicare trustees release 2025 reports,” June 18, 2025.
h. Murphy, H., “Dozens of new AI-powered devices make FDA’s list of approvals,” Radiology Business, Dec. 14, 2025.
i. Bobrowsky, M., et al., “Big Tech’s AI push is costing a lot more than the Moon Landing,” Wall Street Journal, Feb. 7, 2026.
j. Topaz, M., et al., “The coming clinical correction: Why health care needs its AI bubble to burst,” Health Affairs, Feb. 4, 2026.
k. Chang, W., et al., “Hospital trends in the use, evaluation, and governance of predictive AI, 2023-2024,” HealthIT.gov, Assistant Secretary for Technology Policy, September 2025. Predictive AI refers to using statistical analysis and machine learning to classify or produce a risk score for individuals, such as readmission risk prediction, early disease detection, appointment no-show and treatment recommendations.
l. Everson, J., Nong, P., and Richwine, C., “Uptake of generative AI integrated with electronic health records in U.S. hospitals,” JAMA Network Open, Dec. 12, 2025.
Hospitals object to ACA marketplace changes
Proposed changes to the rules of the ACA marketplaces will shift more costs onto hospitals, industry advocates told CMS.
The comments came in response to a proposed rule for 2027 marketplace plans that aimed to stabilize enrollment from 2026 to 2027.
“Hospitals are often the providers of last resort for many patients, and policies that increase patient cost-sharing or reduce network adequacy often shift uncompensated care costs onto hospitals and health systems that are already under significant financial strain,” Ashley Thompson, a senior vice president for the American Hospital Association, wrote in comments to CMS.
More catastrophic plans
Several proposals would expand catastrophic plans, access to which is now generally limited to enrollees 30 and younger. Older enrollees could qualify for such lower-premium, higher-deductible plans through a broadened hardship exemption if they don’t receive subsidies for premiums or out-of-pocket costs.
Such plans could increase deductibles to as high as $15,500 for individuals and be automatically renewed for as long as 10 years. CMS also proposed allowing bronze plans to increase their cost sharing above statutory maximum out-of-pocket limits.
“Rural hospitals or other providers may not be able to collect payment from rural patients with catastrophic or bronze plans because the individuals cannot afford to pay their bills, leading the facility to take on uncompensated care costs,” Alan Morgan, CEO of the National Rural Health Association, wrote in submitted comments. “Ultimately, this becomes a bad debt for the rural hospital or other provider.”
Concerns that the proposed changes would drive increases in bad debt was a common concern among hospital advocates.
America’s Essential Hospitals (AEH) stated that uncompensated care among its member hospitals had reached $11 billion in 2023. And the Catholic Health Association (CHA) noted that member hospitals had more than $25 billion in bad debt in the latest reporting year.
New increases in uncompensated care would come on top of a recent surge in those costs. Year-to-date 2026 bad debt and charity per calendar day is 40% more than year-to-date 2023, according to the latest Kaufman Hall hospital flash report.
“CMS should require robust monitoring and transparent evaluation of the impacts on delayed care, medical debt and hospital uncompensated care,” Lucas Swanepoel, JD, a vice president of CHA, wrote in submitted comments.
Out-of-pocket trend
High deductibles have long been a hallmark of ACA marketplace plans. In 2025, the average deductible was $4,902 for silver plans and the average deductible was $7,186 for bronze plans, according to the Peterson-KFF health system tracker. In 2026, average deductibles increased to $5,304 for a silver plan and $7,476 for a bronze plan.
Those out-of-pocket costs increased in 2026 after Congress allowed COVID-era extra subsidies to expire.
But even when out-of-pocket subsidies were considered, deductibles remained high. The weighted average deductible — including subsidies — across all plans was $2,759 in 2025 before it increased to $2,912 in 2026, according to the tracker.
Any increase in out-of-pocket costs also could exacerbate losses that some health system executives have reported previously from ACA-covered patients who didn’t pay their share of their hospital bill.
Kevin Hammons, CEO of Community Health Systems, told investors in January that ACA marketplace enrollees mainly use the system’s emergency departments and often don’t pay their deductibles or co-insurance.
Network changes
Among a range of proposed network changes, CMS proposed to permit “non-network plans” on the marketplaces and detailed how they could achieve qualified health plan status. Such plans may include those that use reference-based pricing.
Hospitals warned that such plans may provide “illusory benefits” if few healthcare organizations would provide services for its offered payment rates.
“Even if a non-network plan has low premiums, it may not provide meaningful access at the point an enrollee actually requires care,” Charlene MacDonald, president and CEO of the Federation of American Hospitals, wrote in submitted comments.
MacDonald also questioned whether such plans violate federal law.
Enrollment cuts
CMS projected the rule’s changes will lead 1.2 million to 2 million enrollees to drop their ACA marketplace coverage in 2027. Twenty-three million enrollees selected coverage in 2026, although it was not yet known how many effectuated that coverage by starting to pay their premiums. The initial decrease of more than 1 million enrollees in 2026 was substantially less than the more than 5 million decrease this year projected by the Congressional Budget Office if the COVID-era subsidies expired.
Still, hospital advocates urged against finalizing measures in the proposed rule that don’t prioritize preserving coverage.
“Absent such modifications, people could lose access to needed healthcare,” Swanepoel of CHA wrote. “Our members will continue to serve patients. but these enrollment losses will predictably increase uncompensated care, emergency department utilization and financial pressure on hospitals serving as essential safety-net providers.”
Democrat plans
Congressional Democrats have focused on ACA marketplaces in their healthcare pitch to the electorate for the upcoming midterm elections.
Senate Democrats have offered a somewhat vague plan to enact a range of policies, including reinstating COVID-era subsidies for the ACA marketplaces and ban short-term limited-duration plans expanded by the Trump administration.
It also included plans to offer “Medicare-type choices for healthcare,” which could mean creation of so-called public option plans on the ACA marketplaces. Congressional Democrats have previously failed to push such plans through Congress, even when they had large majorities.
“Republicans have spent the past year making these problems worse by passing the largest healthcare cuts in history and pursuing administrative actions that further destabilize health insurance markets,” the Senate Democrats wrote.