





Healthcare Business Trends
Inflation rattles hospital supply chain and labor pool with no end in sight
Strategies for combating inflation include partnering with others to obtain supply discounts and boosting worker mental health.
Published
October 5, 2022
2:37 pm
|
Updated
December 12, 2023
9:09 am
With price inflation driving up healthcare supply and wage costs faster than revenue is growing, hospitals and health systems are feeling a squeeze to become more efficient.

— Susan K. Nelson
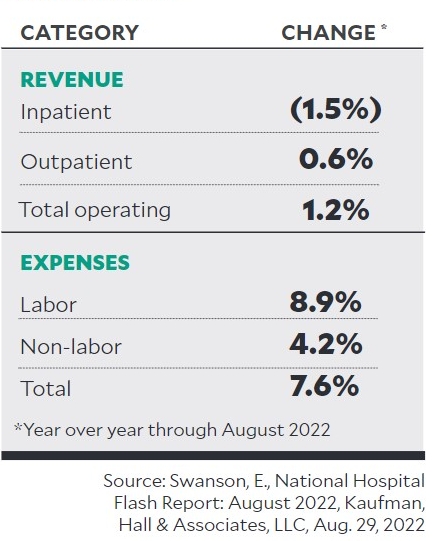
The mismatch between revenue and cost inflation has been dramatic. In the first seven months of this year, hospital revenue climbed 5.5%, while supply and wage costs helped drive hospital total costs 9.6% higher, according to Kaufman Hall’s August 2022 National Hospital Flash Report.
The potential for runaway inflation can be distressing to healthcare finance executives, who have limited tools available to curb the effects of the problem.
“Inflation is impacting [health systems] broadly because they don’t control revenue,” said Kerry Jessani, head of healthcare, higher education and non-profit banking for JPMorgan Chase’s middle market banking and specialized industries business. “It’s all negotiated with insurance companies or the government. Revenue is fixed and costs for labor, supplies and everything else are going up.”
Hospital investments, which can offset negative operational results, have been of little help with the stock market performing poorly (see related story).
In addition to national economy-wide inflation, health systems are experiencing loss of revenue from elective procedures and record-high costs to attract and retain labor, making the inflation fight more difficult.
“We’re having a lot of conversations with health systems around margins,” Jessani said.
Revenue-expense mismatch
For hospitals and health systems, grappling with ongoing cost increases presents obstacles, but it also presents opportunities to adopt new approaches that improve operations.
“This kind of challenge does cause all of us to think more creatively and be more open-minded about solving [problems] in ways we might not have before,” said Susan K. Nelson, CFO, MedStar Health, Columbia, Maryland. “It will force us to think differently about how to get work done, whether it’s through automation or new ways of staffing, and that will be critical both on the clinical side and the non-clinical side. This is a challenging time, but I think it will also be a time of great innovation.”
Bracing for the long term
As inflation continues at high levels, most hospital executives are preparing for a lengthy season of cost pressures.
“Signals show that inflation will last into 2023,” said Margaret Steele, senior vice president, med/surg, Vizient, which is based in Irving, Texas. “The elevated costs of energy, raw materials, logistics and labor will continue to put pressure on pricing of final products. We expect overall market prices for suppliers to increase 4.2% from January 2023 through December 2023.”
While larger economic issues will play a significant role in future costs, the healthcare industry’s response may influence specific impacts.
Inflation threat leads hospital investment managers to proceed with caution
“An ongoing concern is that healthcare supply chain leaders and suppliers, fearing higher inflation, alter behaviors and buying patterns in a way that makes target inflation levels of 2% to 3% unachievable and sustains advances toward elevated inflation levels,” Steele said.
Moving forward, health system leaders must approach the challenges of inflation with patience and creativity.
“Look at your entire cost structure and see where you can save or be more efficient. Ask yourself if you really need to be providing all the services you provide or if you should shift your attention to certain ones,” said Rick Gundling, senior vice president, content and professional practice at HFMA. “It’s a chance to look at your processes with new vigor and build a stronger future.”
Supply chain issues
The pandemic induced major, and likely long-term changes to the hospital supply chain. During the past two years, the healthcare industry went from a system of just-in-time inventory to a supply chain with limited supplies and long delays. As a result, many organizations began stockpiling items to avoid shortages.
“Now that costs are rising, they’re trying to find a balance between keeping enough inventory on hand and staying within budget,” Jessani said. To manage through supply inflation, some smaller and regional hospitals are combining purchasing power to work together with suppliers, Jessani said.
“We’re also seeing more onshoring and nearshoring supply chains; hospitals are looking for supply chains that are closer to home,” she said. “Generally, the supplies may be more expensive, but the quality and assurance is more reliable.”
In addition to partnering with other hospitals to achieve discounts, Jessani recommended that finance executives look within their own organizations for opportunities to increase volume. For example, are they using the same software vendor across the gift shop, parking garage and other points of sale? By standardizing vendors and supplies across the organization, they may be able to get volume discounts.
On the clinical side, supply chain shortages of personal protective equipment (PPE) during the pandemic required considerable collaboration to identify products that would be safe and effective substitutes, said MedStar’s Nelson. Between a workforce that’s been running full-speed for close to three years and clinicians with extra duties to perform, taking on more work centered on efficiency is a difficult ask.

— David Hargraves
Still, there are opportunities to cut supply costs without involving clinical staff. Many hospitals traditionally rely on group purchasing organizations (GPOs) to negotiate supplier prices for them, but those contracts usually don’t cover every cost. For example, most hospitals have about 600 categories of purchased spend; Premier, which acts as a GPO, regularly works with members on about 80 categories, said David Hargraves, senior vice president, supply chain services at Charlotte, North Carolina-based Premier.
“Go look at areas of spend you’ve never really looked at before and consolidate; come up with better strategies and benchmarking,” Hargraves said. “Financial recovery involves all the things you can control that you may not have really looked closely at before.”
Some services, such as contract services, background checks and lipid services, are often contracted at a hospital level rather than a system level. Dig deeper into those categories and find out whether costs can be cut or utilization can be reduced, Hargraves said.
For example, some hospitals order five times more background checks than others because of their internal policies, Hargraves said. So it’s important to consider whether changing utilization or other policies for various spend categories might be an option to help reduce costs.
Wage inflation strategies
During the thick of the pandemic, costs for clinical labor rose dramatically, as more hospitals needed to pay for travel nurses and other contractors to keep their floors staffed, JPMorgan’s Jessani said.
Today, “labor costs are higher across the board, not just in the clinical areas,” she said. “People with transferable skills — such as those working in the financial department, tech department and custodial department — are leaving because they can make more at an Amazon warehouse.”
Trying to keep wage inflation from becoming crippling, especially when coupled with lower revenue, facilities are looking for new ways to retain workers, including the following.
Improve mental health. MedStar Health launched the MedStar Health Center for Wellbeing to support the holistic needs of physicians, nurses, therapists and others who work in the health system. MedStar Health associates support each other during wellness rounds.
Crystal Morales, RN, director of nursing well-being, is hosting “Scrub In,” a monthly podcast focused on well-being for clinical staff.
Nelson added, “We’ve seen a number of nurses leaving for different careers or for nursing outside the hospital setting due to the stress level, so we’re working to help people manage stress.”
Make jobs more enticing. In addition to focusing on mental health and well-being, health systems can work to “expand role flexibility,” said Brian Esser, principal, Sg2. That might include varying locations between acute and nonacute, offering part-time and hourly options, hybrid options for working in-person and virtually, and using float pools and regional or state labor contracts to keep talent local.
Some large health systems are cutting costs on travel labor by contracting nurses within their own systems, said HFMA’s Gundling. This offers new and flexible opportunities to nurses who want them, while reining in exorbitant costs for travel nursing.
Add automation. Making the work more appealing to staffers may improve retention, but by looking for ways to implement automation, hospitals can lower their staffing requirements.
“Position the workforce to work top of license, and actively seek out areas to automate repetitive tasks,” Esser said.
Offload some risk. Another way to offset significant wage inflation is to strengthen your balance sheet by reducing exposure to risk, Jessani said. For example, some of her clients are working to diversify revenue by partnering with other providers to add new services, such as a small system working with a for-profit vendor to offer home healthcare.
By finding partners with different expertise, hospitals can help mitigate the risk of adding new services. In addition, hospitals can partner to expand their geographic footprint, which may result in payer diversification and provide access to additional workforce groups, Hargraves added.