





How a health system can reduce premium labor while building a sustainable workforce
Finance leaders at the academic health system Montefiore Einstein undertook a transformational initiative aimed at reducing its contract labor and overtime costs while also improving the workplace experience for all its nursing and other clinical staff.
Published
May 6, 2026
3:51 pm
|
Updated
June 1, 2026
2:41 pm
Labor costs are the largest single expense for health systems, and reliance on overtime and contract labor can exacerbate these costs. By addressing premium labor, health systems gain opportunities for increasing staff satisfaction and quality patient care, as well as achieving financial sustainability.
Premium labor costs have increased nationally, with contract labor more than doubling between 2019 and 2022.a During the COVID-19 pandemic, according to one report, premium pay contracts and overtime rose to account for nearly 10% of direct labor costs, as nurses faced unprecedented pressures.b Moreover, these pressures also reflected an ongoing trend, as labor expenses as a percentage of net revenue had already been steadily rising, and they have continued to rise since the pandemic.
Behind these figures are real workforce challenges, including nurses covering extra shifts, new hires waiting for system access and leaders navigating contract labor decisions without complete visibility.
To address these challenges, hospitals and health systems should focus on improving their workforce strategy to ensure they have strong onboarding processes, with streamlined scheduling, enhanced data transparency and well-designed operational workflows.
By proactively developing a comprehensive system for managing premium pay labor, health system leaders can avoid situations that require reactive fixes, while establishing a sustainable, resilient workforce that supports both staff and patients.
Too often, health system CFOs and other senior executives view the workforce as a fixed cost to control. Instead, they should treat it as a renewable resource worthy of constant reinvestment. This perspective is important because a health system’s goal should be to design a sustainable model that creates long-term value for the organization and its people. While a focus on reducing premium labor is needed, leaders should strive to do so naturally in a way that inspires loyalty and strengthens retention.
Principles for healthcare leadership change
Health system leaders cannot achieve such an outcome without first embracing the following five principles of leadership that promote workforce well-being.
1 Foster transparency and communication by making data visible at the unit level. Dashboards should extend beyond high-level finance reports. Frontline leaders need real-time visibility into overtime, late punch-outs, contract hours and associated costs. When information is timely, staffing adjustments can happen before problems escalate. Open forums, progress reports and cross-department dashboards encourage shared accountability. When units see systemwide performance, silos break down and collaboration strengthens.
2 Instill financial literacy across levels of leadership. Many unit leaders are experts in patient care, not budgets. Teaching them how scheduling decisions affect costs empowers them to act as stewards of both care quality and financial sustainability. Scenario-based training and weekly workshops can bridge this gap.
3 Streamline onboarding and access. Delays in system access for new hires create ripple effects that lead to overtime and increased reliance on contracts. Coordinating human resources (HR), IT and clinical teams to ensure system readiness on day one accelerates integration and reduces unnecessary premium labor use.
4 Standardize overtime and premium pay contract approvals. Without transparent and consistent processes, approval decisions can vary significantly, often with no consideration given to their financial impact. To facilitate timely and informed decision-making, leaders should design a transparent contract approval process that requires projected costs to be considered before a contract is authorized. This approach promotes accountability and ensures staffing choices are aligned with budgets and patient safety. (See below for a simplified example of a process flowchart.)
5 Hold leaders accountable and celebrate progress. Embedding labor management into performance reviews ensures ongoing focus. Recognizing the units that meet targets reinforces a culture of excellence and motivates teams to sustain gains.
Process for requesting, onboarding and invoicing supplemental nurse staffing
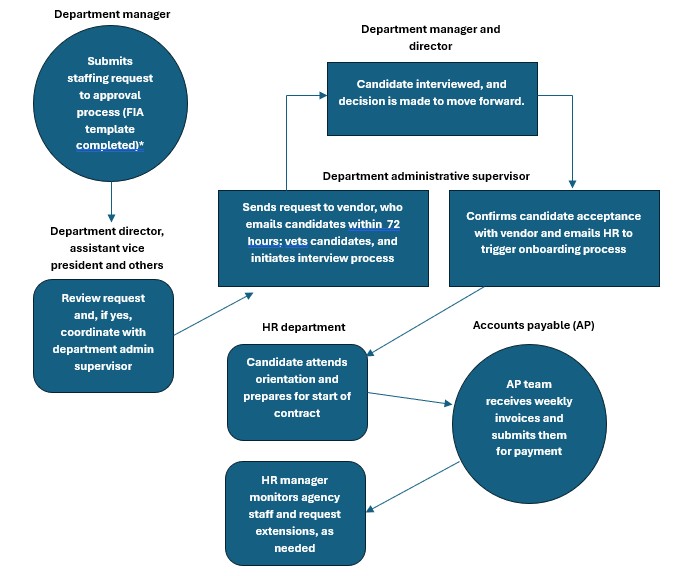
This flow chart is a reduction of the actual process Montefiore uses for fulfilling requests for supplemental nurse staffing and is provided here for illustrative purposes. Hospital leaders can use this basic process as a template for designing a more detailed process that meets their specific needs.
Case Study: Montefiore Einstein
Montefiore Einstein is an academic health system that serves about 3 million people across the Bronx, Westchester and Hudson Valley in New York. Like many health systems, it faces significant labor cost pressures given that labor represents 61% of its total operating expenses. Rather than focusing solely on budget tightening, the health system’s finance leaders reframed this challenge as an operational opportunity to optimize workforce deployment, reduce reliance on premium labor and improve care delivery.
To accomplish these goals, a cross-functional team under executive oversight was empowered to collaborate on and champion a systemwide workforce improvement initiative. Participants included representatives from finance, nursing leadership, HR and other clinical and nonclinical areas. Together, they realized a strategy comprising the following six steps.
1 Simplify access to data. Staff found hospital or IT dashboards in use were too cumbersome to access and interpret. Reports were lost if not checked periodically. To address this problem, simplified dashboards on agency usage and incremental overtime were created to be emailed directly to leaders every pay period — no logins required, no barriers to access. (See examples of Montefiore Einstein’s revised dashboards at the end of this article.)
2 Build financial literacy. Recognizing that some leaders lacked the financial literacy needed to interpret complex reports, ongoing education sessions were implemented to provide leaders with guidance on how to interpret the reports, and the reports were revisited to ensure the data presented in them was accessible, actionable and nonintimidating. These steps contributed to strengthening organizationwide engagement and accountability.
3 Raise hospital leaders’ awareness of vendor contracts and holiday pay. This step had two objectives.
The first was to ensure hospital leaders were informed of which holidays agency vendors recognized to avoid automatic overtime charges under the vendors’ contracts. The leaders were reminded regularly to prioritize internal staff over agency nurses on vendor-recognized holidays whenever possible.
The second was to ensure leaders were aware that some agency contracts charged time-and-a-half for overtime regardless of whether an agency nurse worked additional hours. Senior leaders worked with vendors to revise contracts to make sure overtime reflected actual hours worked, capped at a standard 40-hour workweek.
Montefiore Einstein year-over-year labor expense*
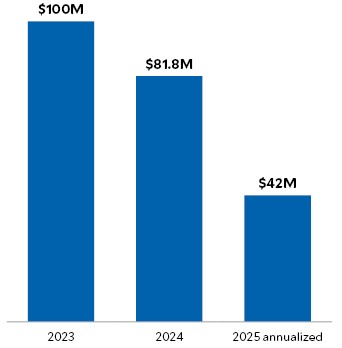
Source: Montefiore Einstein, 2026
4 Bridge the gap between finance and clinical operations. Staff often felt that budget discussions lacked sufficient clinical context, making it challenging to connect financial data with day-to-day operations.
To address this problem, team members met daily to discuss concerns, using hard copies of reports. The team recommended that finance leadership use private coaching, campus-specific meetings and clinician-to-clinician translation of data to help clinical leaders understand not just what the numbers said, but also their impact on patient care.
5 Support accountability with streamlined reporting. Operations leaders faced time constraints that limited their ability to consistently run payroll reports for late punches and attendance. To eliminate access barriers, simplified reports were automatically distributed to leaders after each pay period. During group meetings, educational leadership sessions offered coaching to give leaders an opportunity to confidently discuss their financial performance or other issues with senior leadership, and these points were reinforced with individuals during rounds.
6 Accelerate access for new hires. Despite system changes, barriers continued to delay onboarding, resulting in costly, nonproductive expenses for nurses. Issues such as name changes or promotions required new system access, delaying clinical readiness. Leaders
were encouraged to email concerns to designated team members directly in addition to submitting help desk tickets. This approach ensured that corrections were made in real-time, while the ticketing system still tracked issues for accountability.
Results of the initiative
The premium labor initiative produced measurable, systemwide improvements:
- Contract labor expenses decreased by 32.0% in nine months.
- Nursing premium pay expenditure fell 23.5% across Bronx hospitals in the health system.
- Holiday overtime expenses for contract staff were reduced by 88.3%.
- Respiratory therapy contract labor dropped 53.8% within nine months.
- Incidental overtime (late out punches) decreased by 28.8% among nurses and 60.6% in radiology.
- Recruitment and retention efforts cut RN vacancies by 42.0%.
Overall, Montefiore Einstein was able to reduce contract labor by 68% between 2023 and 2025, improve onboarding efficiency, better engage leaders and achieve more consistent staffing for patients.
Outcomes and impacts of Montefiore Einstein’s workforce improvement strategy
| Outcome | Strategic focus | Impacts |
|---|---|---|
| Sustained 68.6% reduction in contract labor (2023 to 2025) | Workforce management and cost containment efforts | * Reduced reliance on contract labor and controlled related costs * Improved continuity and quality of care due to more consistent staffing * Increased number of regular FTEs, reducing dependency on temporary staff |
| 50% reduction in new hires’ wait times for EHR system access | Streamlined communication/ coordination among HR, IT and the clinical leaders | *Improved orientation efficiencs, enhanced clinical staff readiness and higher employee retention *Improved patient care due to faster onboarding and better prepared staff *More stable FTE workforce from improved onboarding efficiency |
| Improved cost control and staff time management | Enhanced oversight and monitoring of incidental overtime | *Improved use of staff time and management of labor expenses *Reduced fatigue and errors, improving patient safety *Better workload distribution among regular staff |
| Increased financial literacy among frontline leaders | Training and education on budgeting and operational decision-making | *Improved understanding by leaders of budget impacts, enabling more informed decision-making *More sustainable staffing and resource allocation due to better informed decisions *Improved alignment of strategic staffing with patient care needs |
A premium labor playbook for healthcare CFOs
Premium labor is not an unavoidable cost of doing business, nor is it solely a symptom of inefficiency. While some premium labor is necessary to manage clinical evolving demands, prolonged reliance on it often signals deeper workforce challenges that require attention. Montefiore Einstein’s initiative, aimed at reducing reliance on premium labor and overtime, offers an example for other health systems on how they can transform labor management into a sustainable workforce strategy.
Health systems that are planning to launch similar initiatives can benefit from adopting the following 10 lessons learned from Montefiore Einstein’s experience.
1 Use data-driven decision-making. Leverage real-time analytics and targeted reports to identify labor cost drivers and inefficiencies.
2 Engage frontline leaders. Train leaders on financial literacy to empower informed staff and budget decisions.
3 Optimize staffing models. Align schedules with patient demand to minimize unnecessary overtime and contract labor.
4 Streamline onboarding. Coordinate HR, IT and clinical teams to reduce delays in system access and speed up new hire productivity.
5 Standardize overtime and contract approvals. Implement clear approval workflows to control premium pay usage and avoidable costs.
6 Foster cross-departmental collaboration. Break down silos among recruitment, HR, finance and operations to improve workforce planning and problem-solving.
7 Implement continuous improvement cycles. Use Plan-Do-Study-Act or similar methods to iteratively test, measure and refine labor strategies.
8 Promote transparency and accountability. Share labor metrics regularly and hold leadership reviews to maintain focus and drive improvements.
9 Balance cost savings with quality and well-being. Avoid quick fixes that harm care continuity or increase burnout; focus on sustainable workforce stability.
10 Scale successful practices systemwide. Expand proven strategies beyond pilot areas to maximize cost savings and operational efficiency.
Fundamentals for a strong healthcare workforce
The takeaway is clear: Reducing premium labor requires more than tightening budgets. It demands that leaders bridge finance and frontline operations, align departments around shared goals and build a culture of accountability and empowerment. When this alignment takes hold, health systems not only reduce costs but also strengthen staff engagement, improve retention and elevate patient care.
An even more fundamental takeaway from this initiative for Montefiore Einstein: The
key ingredient for success was the interdisciplinary collaboration and sustained commitment
of all team members from every level of the health system.
Footnotes
a. American Hospital Association, “Hospital contract labor costs surge amid workforce shortages,” March 8, 2023.
b. Myerson, S., “Nine tips for reducing your premium labor spend,” ECG Management Consultants, Dec. 3, 2020.
Authors’ note
The authors would like to acknowledge Peter Semczuk, DDS, MPH, Montefiore Einstein’s regional senior vice president, and the operations and nursing teams for their contributions toward the development of this article.